This curated collection of case studies, developed by the Harvard Ministerial Leadership
Program, offers practical insights into transformational leadership including key aspects
of political navigation, policy implementation, and reform, drawing directly from the
experiences of government Ministers.
Designed to bridge theory and practice, these
studies illuminate real-world challenges, present innovative solutions across diverse
sectors, and support informed decision-making. They serve as essential tools for
translating knowledge into impactful policies and driving meaningful change.
In February 2017, Dr. Matthew Opoku Prempeh was appointed Ghana’s Minister for Education. From the get-go, the President of Ghana, President Nana Akufo-Addo, tasked him with delivering Free Senior High School (Free SHS) in the country, a program that would provide free education, paying for a total of 41 items, including tuition, meals, textbooks, and boarding for Ghanaian children qualified for secondary education.
This task was challenging. More than 100,000 additional students, who should have been attending senior high school, needed to be absorbed into the system annually. Classrooms, dormitories, science labs, ICT labs, and workshops for technical and vocational education and training (TVET) were in short supply, in addition to teacher shortages and poor-quality teaching in the secondary education system. There was also political opposition. Many in the opposition cited infrastructure gaps and concerns over quality teaching as reasons why Free SHS should not be on the Ghanaian agenda at the time. Nonetheless, by September 2017, just seven months after his appointment, Dr. Matthew Opoku Prempeh launched Free SHS nationwide and, consequently, increased SHS attendance.
How did Ghana manage to deliver Free SHS nationwide so quickly? What lessons can other political ministers draw about leadership, resource mobilization, stakeholder engagement, and organizing for results? This case study, built from extensive conversations with Minister Prempeh and his collaborators, uses the Harvard Ministerial Leadership Program’s framework to unpack the strategies, challenges, and decisions behind the Free SHS program led by Minister Prempeh, while inviting ministers to reflect on how to apply these lessons in their own contexts.
Leading with Clarity
Minister Prempeh’s appointment was not a surprise; President Akufo-Addo pledged free secondary school in his manifesto. “In 2012, during the election petition, the President told me that if we won, he wanted me to be Minister for Education,” Minister Prempeh recalls. “When we finally won in 2016,” he said, “For you, I haven’t changed my mind.” Despite his background as a medical doctor, a path somewhat unconventional for leading a Ministry of Education, Minister Prempeh accepted the President’s challenge and the confidence placed in him to lead Ghana’s education sector and achieve the President’s vision.
President Nana Akufo-Addo’s mandate for Minister Prempeh was clear. “He had looked at his team and said I had the energy and intellectual depth to handle his most important legacy policy: free secondary education,” says Minister Prempeh. Thus, he went on to adopt the President’s goal as his own mission.
The following quote from President Akufo-Addo’s speech, when launching the free SHS program in September 2017, and as highlighted by Minister Prempeh, is what largely motivated him to ensure the success of free SHS:
“A government may not be able to make every citizen rich. But, with political will and responsible leadership, a government can help create a society of opportunities and empowerment for every citizen, and I know no better way to do so than through access to education.”
After his swearing-in to office, the first person Minister Prempeh spoke to about his role as a government leader was the President himself:
“I went to him for a series of engagements to help me get a deeper and better understanding of his vision for education in Ghana, in general, and the free SHS, in particular. I also had discussions with the Vice-President, Dr. Mahamudu Bawumia, who had been with and shared the President’s vision right from the onset in 2008. He indeed helped me reshape my thoughts and psych myself up for the task ahead.”
Moreover, Minister Prempeh immediately set expectations with the President. “I told him, ‘This is life-transforming. What I need most is your backing 24/7 until we get it done.’ He promised, and he delivered. The President was with me throughout, meeting frequently, even deciding what would go into the Free SHS package,” he says.
Minister Prempeh saw his role as Minister for Education as more than a job. “I was in politics for the long term. I could not fail. Failure would not only kill the policy but also destroy my career. I treated this as a mission, not just a position.”
Clarifying Priorities
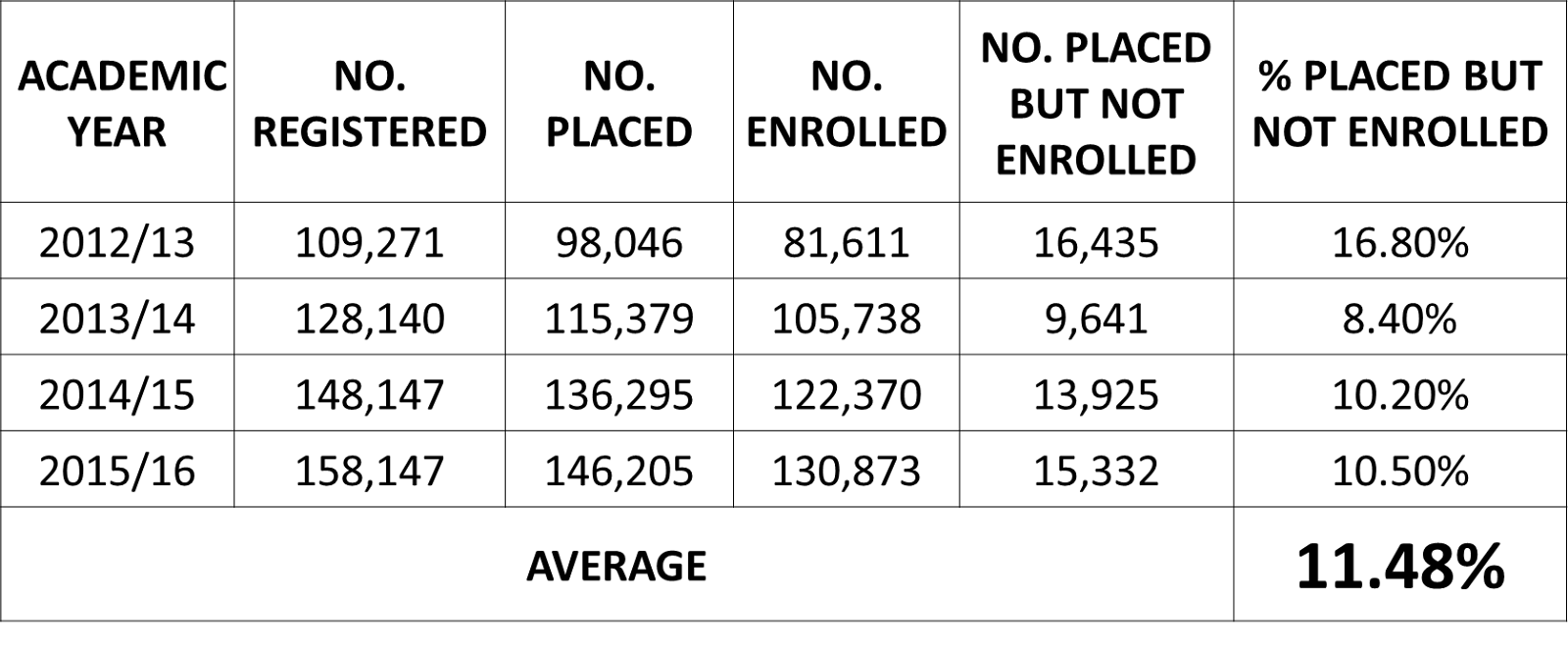
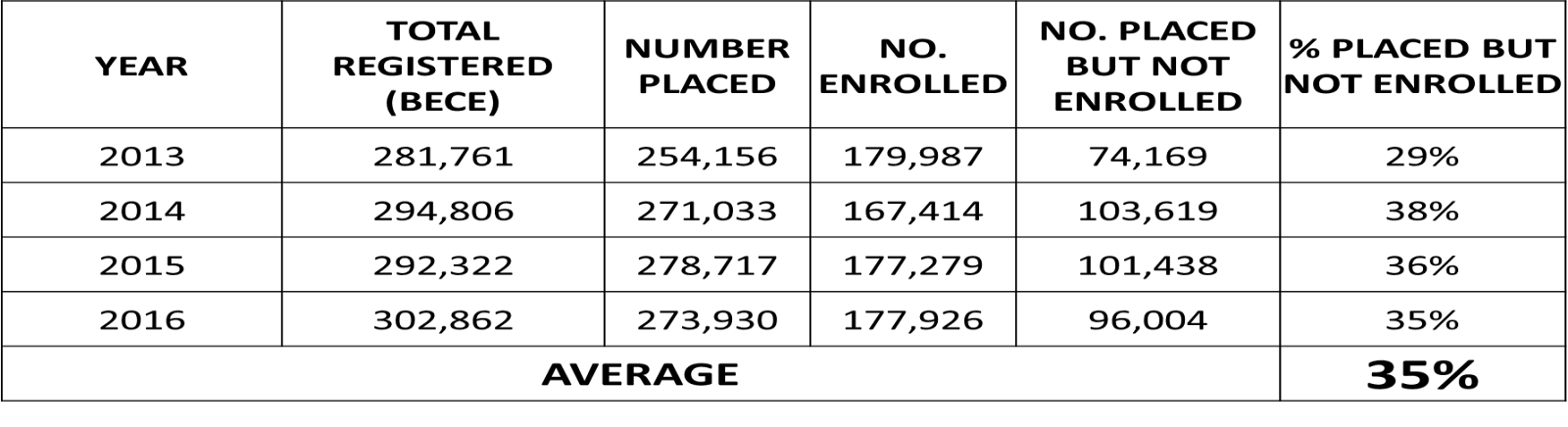
Data available to the Ghana Education Service (GES) and the Ministry for Education, at the time, pointed to the fact that the biggest barrier to SHS (Secondary High School) enrolment in the country was financial. Many did not attend SHS because they could not afford its cost. This was evidenced by the enrolment rates analysis of pre-Free SHS data when disaggregated for learners benefiting from the Northern Scholarships, and learners in the Southern part of the country who were not beneficiaries of the scholarship or bursary.
TABLE 1: NORTHERN SCHOLARSHIPS ADMISSIONS AND PLACEMENT TRENDS
TABLE 2: SOUTHERN ADMISSIONS AND PLACEMENT TRENDS
Hence, “The free SHS was rolled out primarily to address inequality among students, through the removal of cost barriers whilst enhancing quality. We committed to creating a fair, safe and prosperous future for our citizens by providing equal opportunities for all,” Minister Matthew says. Moreover, to be effective in delivering free SHS, him and his team set four clear priorities and anchored them on four main pillars:
Removal of Cost Barriers: Remove cost barriers through the absorption of fees approved by the Ghana Education Service (GES) Council.
Access and Expansion of Infrastructure: Expand physical school infrastructure and facilities to accommodate the expected increase in enrolment.
Improvement in Quality and Equity: Improve quality through the provision of core textbooks and supplementary readers, teacher rationalization and deployment, etc.
Development of Employable Skills: Improve the competitiveness of Ghanaian Students to match the best in the World.
There is a reason why Minister Prempeh set priorities. From his perspective, priorities needed to be clear and set because “the goal was simple but massive”. This goal meant “full access to SHS up to age 18, at no cost, while maintaining quality. That meant new dormitories, classrooms, books, and teachers, all in months, not years.”
Moreover, these priorities drew on Ghana’s constitutional directive to expand free education as the economy allowed, and on global and continental targets, including SDG 4 (Ensure inclusive and equitable quality education and promote lifelong learning opportunities for all) and the African Union’s Agenda 2063.
Defined Legacy Goal
Minister Prempeh and President Akufo-Addo did not just frame Free SHS as a policy. They framed it as a legacy that would shape their country. In Minister Prempeh’s words, “over 100,000 junior high graduates could not continue to SHS each year, primarily due to cost. In northern Ghana, where partial scholarships existed, only 11% of qualified students missed school. In the south, without scholarships, 35% could not attend.” Therefore, reducing cost and improving access to secondary education were a priority and the transformative legacy goal the minister wanted to achieve. His own experience growing up in Ghana motivated him to work on this goal. For him, “the shortest bridge [he] ever crossed was between poverty and prosperity, and that bridge was education. Without it, the gap is a gulf. With it, the bridge is short.” President Akufo-Addo said:
“By free SHS, we mean that in addition to tuition, which is already free, there will be no admission fees, no library fees, no science center fees, no computer laboratory fees, no examination fees, no utility fees. There will be free textbooks, free boarding, and free meals and day students will get a meal at school for free.”1
Defined Metrics and Delivery Unit
Minister Prempeh was appointed in February 2017, and Free SHS had to be launched in September 2017. With just seven months to launch, data monitoring and accountability were critical. Thus, Minister Prempeh constituted an advisory team, established a Free SHS Secretariat and a Delivery Unit, among other actions, to track every operational detail. He built these teams by closely collaborating with technical experts, such as Professor Kwasi Opoku-Amankwa, the Director-General of GES (Ghana Education Service), and indeed with heads of all the 26 agencies and their affiliates of the Ministry of Education. The GES is an agency under Ghana’s Ministry of Education that oversees the implementation of government policies to ensure that all Ghanaians receive formal education.
Together, “We built dashboards for each school,” Minister Prempeh explains. “We tracked classrooms, dormitories, textbooks, teachers, and feeding programs. We used a traffic-light system.”
Professor Opoku-Amankwa, who also acted as the technical advisor to the Minister for Education and the Government of Ghana on all matters relating to pre-tertiary education, explains how essential it was for the SHS Secretariat and delivery unit team to use data-driven tools to monitor free SHS outcomes and keep the program on track and accountable. He says:
“We put everything that we were doing into a table, and then we labeled them red, gold, and green. If it was green, it meant it was done. If it was red, it was outstanding. If it was gold, we were working on it, and we gave reasons for each status.”
This “traffic light” system created rapid feedback loops, with weekly updates to the Cabinet and, when necessary, escalations to the President’s office. It also created visibility across all program areas, from curriculum reforms and infrastructure development to teacher training and ICT rollout. By combining operational tracking (traffic light tables) with impact indicators (access, performance, and equity), the SHS program was able to identify gaps early, adjust quickly, and clearly communicate progress, setbacks, and program-related updates to stakeholders.
Cross-Collaboration & Stakeholders Mapping and Engagement
With a clear understanding of the President’s vision, and further details from the Vice President, Minister Prempeh’s next move was building a coalition across government and society to successfully implement free SHS. He says, “Ministers don’t connect to graphs; they connect to stories. So, we told a story about why Free SHS mattered, but we always backed it with hard data.” Therefore, he went on to have a series of engagements with virtually all colleague Cabinet ministers. He says:
“My view was that education affects and relates to all ministries. Every ministry has an input into education development. For example, I needed to secure the funds for free SHS from the Ministry of Finance. I had to talk to the Minister for Food and Agriculture on issues relating to food and manciple, while I talk to the Interior Minister on security and safety matters on our school campuses. There is a whole unit on school health programme in the Ghana Education Service. The unit works closely with a similar unit in the Ghana Health Service. I needed to talk to my colleague Health Minister, to ensure a seamless and collaborative work between the units.”
Professor Opoku-Amankwa added:
“The hon. minister used data and evidence-based research to effectively make a case for us all to participate fully in the President’s mission. Through a series of meetings and engagements, we developed a shared vision and implementation framework and communication plan to guide us. The hon. minister also communicated with us, the team, effectively the key objectives of the Free SHS and how free education has insured the success of many nations including the USA and most developed countries.”
Moreover, “The President himself met with the unions,” Minister Prempeh says. “We made sure everyone understood the vision, even if they didn’t fully agree.”
Minister Prempeh highlights the key stakeholders he included in this mission as follows:
“I also needed the buy-in of my caucus members of parliament and the leadership and communication team of the governing party – the New Patriotic Party (NPP).”
“I went beyond these internal party groups to engage the parliamentary committee on education.”
“I constituted an advisory team which included a group of eminent educationists, academists, technical experts and entrepreneurs, industrialists.”
“At the level of the ministry, I made sure we had a shared vision. I engaged and subsequently involved the leadership and management teams of all the twenty-six agencies under Ministry of Education. We worked together through a series of in house and out of office meetings to plan out the various reforms beyond the free SHS: curriculum reforms, teacher professionalization, infrastructure audit and upgrade, provision of logistics and equipment to support teaching and learning, enactment of enabling Acts of Parliament, etc.”
“The education sector unions and associations: GNAT, NAGRAT, CCT, CHASS, CODE, APTI, were all roped in.”
“The development partners – the World Bank, USAID, FCDO, (DfiD then), JAICA, etc., who are our key partners, were deeply involved right from the conception stage of our journey.”
“I equally engaged a good number of the civil society organizations in education, as well as those whose activities relate indirectly to education, were engaged.”
“As a strategy, I arranged for the leadership of the key stakeholders, such as the education unions, to meet and interact with the President on his vision for education and his national development agenda generally. These engagements helped a lot to ease the various agitations that were mounting.”
“Put the head of the union in the cabinet for them to understand that indeed this was government priority Number 1, and the whole cabinet was behind it, including the President, 100%.”
“The media was not left out. Beyond the periodic press conferences that were held to brief the media on the ministry’s activities. I tasked my deputies and agency heads to engage in frequent media programmes to inform and educate the public on the various reforms.”
A core reason Ghana’s Free SHS program succeeded was the deliberate strategy to map, engage, and coordinate stakeholders across every level of the education system.
This mapping was not just symbolic; each group was given a role in decision-making and communication. For example:
Teachers’ unions brought representatives into program committees.
School leaders (headmasters and headmistresses) participated through their associations.
Parents and the media became partners in public updates.
Retired educators and eminent experts formed advisory circles to shape vision and gather buy-in.
Professor Opoku-Amankwa added that “whatever vision was crafted became a shared vision. People were given various responsibilities, so it wasn’t just a government program, it became a national commitment.”
This approach also neutralized opposition and improved trust:
“We updated the public as frequently as we could. And with the unions involved, we had a seamless start.”
By mapping and activating 26 agencies under the Ministry of Education and multiple external groups, the GES and Ministry created a delivery network that could overcome skepticism, handle crises, and sustain the program beyond one government. Professor Opoku-Amankwa says:
“There wasn’t a single person who worked in the ministry who didn’t have something to contribute. Even the security person at the gate was expected to know the basics about the program.”
Political Navigation
Like in many countries, there was a strong political opposition in Ghana, and the opposition was intense. From Minister Prempeh’s perspective, “The opposition wanted to win the next election. They refused to support anything, held press conferences, and asked, ‘Where will students sleep? What will they eat? Where will you find the money?’ They even used my predecessor’s handover notes to highlight every gap.”
Infrastructure deficit was one of the pronounced challenges of the education sector in general, at the time the New Patriotic Party (NPP) took over the reins of government in January 2017. The opposition, then, the National Democratic Congress (NDC), argued that Ghana was not ready yet for the free SHS, insisting that free SHS could not be started because there was a huge infrastructure deficit that needed to be resolved first. But then, President Akufo-Addo and his government asked a simple question:
“Whose child should be left behind, while we build infrastructure to catch up?”
Minister Prempeh’s strategy was to out-communicate. “We met unions, parents, civil society, the press, anyone who would listen. We shared data, corrected misinformation, and gave regular updates. Because we had engaged early, people saw through the politics. By creating shared ownership, this goal gained legitimacy and avoided internal resistance.”
A key philosophy in Minister Prempeh’s leadership, according to Professor Opoku-Amankwa, was making sure every person in the ministry and every stakeholder could represent this program, even at the front gate of the Ministry. This ensured consistent messaging and built pride and ownership throughout the system.
In Minister Prempeh’s words:
“Criticisms were inevitable and were to be expected for such a grandiose pro-poor social intervention programme in a cash-strapped developing country such as Ghana. We were, however, resolved to execute the President’s vision of free SHS at all costs. We used the media more to educate and inform the general public on the importance of free secondary education. Perhaps we held more press briefings than any other ministry at the time.”
And delivery depended on trust and collaboration across diverse groups:
“Everybody who is a stakeholder was contacted, and they were represented in all the decisions that we made… teachers’ unions, heads of schools, parents’ associations, the media, and even retired professors and educators. Whatever vision was crafted became a shared vision,” Professor Opoku-Amankwa says.
By creating shared ownership, the program gained legitimacy and avoided internal and external resistance.
Delivering a nationwide program like Free SHS required more than plans, it demanded a mindset that treated every challenge as an opportunity to innovate, especially while dealing with multiple stakeholders. Professor Opoku-Amankwa described how a problem-solving culture, driven by the Minister and embraced by the entire team, became a cornerstone of their success:
“Anytime there was an issue, we discussed and found solutions. What he [minister Prempeh] was very much interested in was options… we would look at the strengths and limitations of each alternative before taking it to Cabinet for approval.”
This proactive, options-driven approach allowed the team to adapt quickly, whether it was managing unexpected over-enrollment through the double-track system or keeping education alive during the early months of the COVID-19 pandemic via Wi-Fi, remote teaching, and carefully managed schools reopening.
Ultimately, political leadership was decisive. “The President drove this himself. He didn’t just sign off; he chose the Free SHS package, defended it publicly, and ensured funding. Without that will, it would have failed,” Minister Prempeh recalls.
Key Levers: Infrastructure and Teachers’ Capacity
In Minister Prempeh’s words:
“The first thing I did was to put a team together to do a study to apprise me with the state of education in the country. This included a thorough infrastructure audit for the entire education sector, however, with emphasis on SHS. The handing over notes of the then outgoing Minister for Education, Professor Jane Naana Opoku Agyemang (current Vice President of Ghana), also listed a litany of infrastructure challenges.”
“On the basis of the audit report, I worked closely with the Ghana Education Trust Fund (GETFund) and other fund sources from our development partners, to construct over 800 senior high school infrastructural projects between 2017 and 2021, covering:”
200 classroom blocks
200 new dormitories
350 science and computer laboratories were either newly built, retooled, reequipped or refurbished, and provided with requisite chemicals for practical work
Construction of TVET workshops and school administration blocks
60 assembly halls, as well as dining halls, toilet facilities and teachers’ bungalows
“We equally provided furniture: bunk beds, classroom desks, laboratory equipment for all the newly constructed structures, as well as procured additional furniture for almost all the senior high schools. We also made provision in the free SHS budget for maintenance of buildings, furniture and equipment.”
“We also provided numerous resources and incentives to support teaching and learning:”
Math and Science training for SHS teachers
Core Textbooks: English language, mathematics, general science and social studies, for all SHS students
Special annual training for teachers in the four Core Subjects:
English
Mathematics
Science
Social Studies
Paid Teacher Motivation/Academic Intervention allowance to teachers
Remedial packages delivered to all students
Support for low-performing schools
On-time payment of subventions
“Our strategy was not on rural schools per se; the strategy was to look up for underperforming schools. The MOE, GES, and the development partners – the World Bank, under the ‘secondary education improvement project’ (SEIP) had identified about 30% of our secondary schools across the country as underperforming. The SEIP supported the schools with infrastructure, grants, and training in accountability for heads and programmes for teachers to improve teaching and learning.”
Resource Mobilization
The cost of Free SHS was around 450–500 million US dollars annually for subsidies, textbooks, feeding, and teacher incentives, plus hundreds of millions more for infrastructure.
Funding strategies included:
Allocating 9% of Ghana’s oil revenues to education.
Securitizing the GETFund, Ghana’s education fund, for infrastructure.
Leveraging World Bank and development partner support.
These resources funded 200 dormitories, 200 classroom blocks, 350 science labs, 600 assembly halls, new furniture, textbooks, and teacher pay raises of up to 80%, alongside extra allowances for tutoring students who needed tutoring. Minister Prempeh explains that:
“The government made funding available from the oil proceeds. About 9 percent of the country’s oil proceeds were earmarked for free SHS and the education sector. However, to secure funds upfront, the Ministry of Finance accepted my proposal to securitize the Ghana Education Trust Fund (GETFUND) receivables to secure the Ghana cedi equivalent of USD 1,500,000,000. This move helped to raise funds to support infrastructure development and the provision of tools and equipment for the sector.”
Moreover, implementing Free SHS required significant financial, human, and institutional resources, often in the face of skepticism, even within government. In Professor Opoku-Amankwa’s words:
“Even within the Government, we had initial challenges. There were ministers, including the finance minister at that time, who thought that we were probably rushing. There were times that we had a feeling we were being denied the resources to run the place.”
Despite this, the Minister for Education found ways to secure the necessary support, Professor Opoku-Amankwa shared. “He found a way of going around to get the right resources to move the entire programme.”
Resource mobilization went beyond just budget allocations. The team activated multiple ministries and agencies to contribute:
Ministry of Health for school health programs and food safety.
Ministry of Agriculture to secure food supplies.
Engineers and infrastructure teams to expand school capacity.
ICT investments, including Wi-Fi installations, to sustain learning during COVID-19.
This whole-of-government and whole-of-society approach ensured the Free SHS program had the financial backing, facilities, human capital, and technical support it needed, even when resources were scarce or contested.
Organizing for Effective Delivery
As Director General of the Ghana Education Service (GES), overseeing over 350,000 teachers and staff and more than 6 million students, Professor Opoku-Amankwa described how effective organization was central to the success of Ghana’s Free SHS. “My duty was to ensure the seamless and successful implementation of any program or policy that the Minister and the Government put in place. I was almost like a co-pilot to the Minister as far as the implementation of the free SHS was concerned,” he says.
Professor Opoku-Amankwa coordinated a vast network of Regional Directorates, Directors, District officials, and School heads. He emphasized the importance of clear roles and communication. “We had about 700 secondary schools across the country. Regional Directorates, Regional directors, District directors, and then the Heads of the schools. All that structure had to be aligned.”
This structure allowed the GES to act as the implementing engine for policies, while the Ministry handled strategy and policymaking.
Minister Prempeh also credits the Harvard Ministerial Leadership Program for sharpening his approach to his role. After his appointment in February 2017, he was invited to the Harvard Ministerial Leadership Program in June 2017, where he participated in the Sectoral Ministers Forum to go through the Program curriculum and access its resources. Minister Prempeh took full advantage of the opportunity, and as he put it:
“Harvard opened my eyes to delivery units, stakeholder mapping, and rapid implementation. It showed me how to track every detail, so nothing slipped through. That’s how we launched Free SHS in just seven months. My participation in the Harvard Ministerial Leadership Program gave me top notched knowledge and skills in leadership, governance and management. I got the opportunity to hear and learn at first hand the success stories and the pitfalls to avoid from a wide range of current and former ministers from across the globe. The Program also provided a network and a pool of experts to contact in times of need. Overall, the Program gave me the needed confidence to execute my mandate as Minister for Education successfully.”
Moreover, Minister Prempeh credits his knowledge in project management for leading with clarity and organizing for effective delivery. He says:
“Planning, preparation, communication and teamwork, and various leadership principles and stories, and case studies from my Harvard Ministerial programme, came in handy. The ‘traffic light system’ helped me a lot to monitor and track progress of work.”
Results: Launched Free SHS
Free SHS outcomes validated the effort. Impact was measured not only by implementation milestones, but also by student outcomes:
“When the first Free SHS cohort wrote their exams in 2020, 411 of our students scored top ‘A’ grade in all 8 subjects, out of 465 in all of West Africa. Ghana won all top three positions of the 2020 and 2023, won second and third positions in 2021, and in 2022, won the first and second positions of the West African Examinations Council’s International Excellence Awards.”
The positive outcomes have also reflected in the academic performance of the first four cohorts of the Free SHS who completed in 2020, 2021, 2022 and 2023. Analyses conducted on performance trends in the core subject areas over a nine-year period, shown that the WASSCE results of the Free SHS 2020, 2021 and 2023 cohorts, scored above 50% in all four core subject areas, making their prospects for enrolment into tertiary institutions higher than in previous years.
TABLE 4: PERCENTAGE OF CANDIDATES OBTAINING A1 – C6 IN THE CORE SUBJECTS
SUBJECTS
2015
2016
2017
2018
2019
2020
2021
2022
2023
English Language
45.2%
51.6%
52.24%
46.79%
49.06%
57.34%
54.08%
60.39%
73.11%
Mathematics
32.4%
33.1%
41.66%
38.15%
64.23%
65.71%
54.11%
61.39%
62.23%
Integrated Science
28.7%
48.3%
52.89%
50.48%
62.94%
52.53%
65.70%
62.45%
66.82%
Social Studies
57.4%
54.5%
42.52%
73.25%
75.36%
64.31%
66.03%
71.51%
76.76%
Specific to the implementation of the Free SHS and the passage of the following two Acts were very significant: the Education Regulatory Bodies Act, 2020 (Act 1023) strengthened and enhanced the regulatory roles of the National Teaching Council, the National Council for Curriculum and Assessment, and the National Schools Inspectorate Agency. The Pre-Tertiary Education Act, 2020 (Act 1049), on the other hand, established the Ghana TVET service as a new agency to cater for the TVET sector. The Act also defined FSHS to include TVET.
In Professor Opoku-Amankwa’s words:
“Dr. Matthew Opoku Prempeh provided what I will call results-oriented leadership. He ensured that every team member had the resources required to enable them to deliver. He delegated effectively, monitored and did formative and summative evaluation of the programme. He devised what he called the traffic light system to effectively track implementation and the performance of each team member. Chaired meetings and gave support and guidance to the team.”
And because of the focus on this transformative goal and the strategic approach, Minister Prempeh says, “In the first year of Free SHS, dropout rates in the South fell to match the North. Over 100,000 students each year, who would have been on the streets were now in school.”
References
1 Borgen Project. “Ghanaian Government Supports Free Education Program – the Borgen Project.” The Borgen Project, 5 Oct. 2017, borgenproject.org/free-education-program/.
Benita Kayembe,
Senior Research and Program Coordinator
In the wake of the covid-19 pandemic your country is facing national debt totaling 50% of annual GPD – which the IMF judges to be almost unsustainable – and persistent deficits, which reached 8% of GDP in 2020, and remained at 3% of GDP in 2023. Those deficits have reflected increased spending – owing to the pandemic and high global fuel and food prices – as well as reduced revenues. Your country does not have access to significant resource revenues, with the economy reliant on agricultural production, a nascent but small industrial sector, a large but relatively simple services sector and a recently growing construction and real estate sector.
Prior to the pandemic non-resource tax collection was 14% of GDP – somewhat above average for LICs – but revenue fell to 12.5% of GDP during the pandemic, and has only recently returned to 13% of GDP. Revenue collection in the country is heavily dependent on the VAT and excise taxes (7% of GDP), with the remainder made up of trade taxes (1.5%), corporate income taxes (2.5%) and personal income taxes (2%). Prior to the pandemic revenue collection had increased from 11% of GDP to 14% of GDP over a decade, which included the creation of a semiautonomous revenue authority, significant improvements in pay for senior tax officials and progress with digitalization, with the government having introduced several core modules of the international SIGTAS IT system.
You are facing major pressure to expand revenue collection, which was an important priority in recent elections, held six months ago. The newly elected President emphasized three possible areas for strengthening tax collection. First, strengthening the taxation of the informal sector and broadening the tax net. Second, curbing corporate tax abuse by multinational companies. Third, strengthening the taxation of the wealthy. She has not focused on raising or strengthening value added taxes, owing to a concern that they may unpopular with her political base in the aftermath of the pandemic.
In each area she emphasized that these reforms were about improving fairness, so that everyone pays their fair share. She promised that new revenues would be translated not only into reduced debt, but expanded spending on health and education. Backed by those promises, her push for stronger tax collection appeared to enjoy significant public support.
Setting Priorities
The President has asked you to build a strategy for strengthening revenue collection. You have asked your advisors to assess the revenue potential of the alternative approaches, and to offer advice on potential strategies.
With respect to revenue potential they have advised that:
Taxing the Informal Sector: While there is a large informal sector which could be taxed more, there is a need to target the small subset of larger firms and wealthier individuals in the informal sector with significant revenue potential. Otherwise, you risk devoting scarce administrative resources to very small taxpayers with limited revenue potential.1
Corporate Tax Abuse: There is a clear need to strengthen taxation of multinational corporations. However, because of the small number of such firms the achievable revenue potential is likely not more than about 0.75% of GDP at best, while success may be challenging owing to the complexity of administering international tax rules.2 There is also some evidence that tax exemptions and incentives have been granted to influential businesses with little justification, which could offer immediate revenue potential and be publicly popular. That said, the overall revenue potential is unlikely to exceed about 0.25%, or at very best 0.5%, of GDP.
Taxing the Wealthy: More effectively taxing the wealthy holds the greatest revenue potential. Personal income tax collection is dramatically below levels in higher income countries (about 9% of GDP) and also well below other high-performing LICs and LMICs (4-5% of GDP). In turn, almost all personal income tax revenue (94%) is collected through withholding on salaries, with negligible collection from capital gains, self-employment income, rental income or inheritance taxes. Property taxes are also extremely weak (0.05% of GDP vs 2% of GPD or more in high performing OECD countries), despite high levels of investment in the real estate sector.
They have recommended a primary focus on strengthening taxation of large and wealthy taxpayers, noting both revenue potential and the potential to increase equity – an important priority for the President. To do so, they have recommended (a) renewed efforts to identify large taxpayers in the informal sector, to expand the tax net, (b) strengthening collection of existing taxes on the wealthy – especially personal income taxes and property taxes – for which there is evidence of major gaps in collection, and (c) a specific effort to investigate existing tax incentives and exemptions to large firms to identify unjustified revenue losses.
Existing Challenges
Following that initial advice, you asked your advisors to conduct an assessment of the drivers of weak existing taxation of the wealthy. Their assessment highlighted the following:
Policy: Policy around personal income taxes – including capital gains taxation and rental income taxation – underwent a significant update in 2019 and is consistent with what is considered international best practice and with regional norms. The policy framework for property taxes is similarly aligned with international practice, and could support reform modelled on that pursued successfully by neighboring countries.
Gaps in registration and compliance: Collaborative research between the national revenue authority and an external think tank that was conducted in 2018 highlighted major gaps in registration and compliance by wealthy individuals in the country, even where those individuals were well known or easily identified. Illustratively, they found that3:
Only 5% of company directors in the country remitted any personal income tax.
Of 16 individuals who paid more than $150,000 in customs duties in the prior year, only 2 remitted any personal income tax.
Among the 60 top lawyers in the country, as identified by the industry association, only 17 remitted any personal income tax.
Among 71 top government officials who were known to own significant commercial assets, only a single person paid any personal income tax.
Limited data sharing: Many countries rely on data sharing both with other government bodies (e.g. public procurement, land ownership, construction) and private actors (e.g. banks, digital financial services, stock exchanges) to identify wealth and income for tax purposes. However, existing legislation in your country sets very high standards of evidence to be able to access data. Meanwhile, other government institutions have often not prioritized, or been resistant to, sharing data. This has made data sharing very limited in practice.
Weak property taxation and knowledge of property assets: Heavy investment in real estate by elites is believed to be a major driver of rising real estate prices, and a major source of untaxed rental income. However, government knowledge of land ownership and values is limited by an incomplete and out of date national cadaster, highly ineffective property valuation and extremely weak property tax administration. As a result, property tax revenue are extremely low even by regional standards, while limited knowledge of property ownership and values has affected the ability of the government to identify wealthy taxpayers and to collect rental income taxes.
Challenges accessing overseas wealth: Cross-country data suggests that a significant share of the wealth of national elites is held offshore, as the average for similar countries is estimated at 30-40% of wealth.4 Recent leaks from tax havens have, in fact, highlighted the names of several wealthy individuals from your country. However, as of now no action has been taken against those named in recent leaks, while the country does not have systems in place to participate in automatic exchange of information (AEOI) for tax purposes in order to access data about wealth held overseas by citizens.
Limited audit capacity: Tax authorities struggle to bring cases against wealthy individuals given limited internal audit capacity, and the ability of those wealth individuals to rely on complex avoidance schemes. This is exacerbated by significant challenges with staff retention, as auditors are often targeted for recruitment by accountancy and legal firms.
Reform Options
In light of that analysis your advisors have highlighted several potential priority actions, highlighting some of the opportunities and costs of alternative approaches.
Creating a High Net Worth Individuals (HNWI) Unit: In recent years a number of countries have created specialized units for taxing wealthy individuals, alongside existing Large Taxpayer Units that focus primarily on large businesses. They have aimed to provide more personalized engagement with wealthy taxpayers, while also strengthening audit capacity and data collection/sharing. International experience suggests significant immediate success in identifying wealthy taxpayers, but that increasing compliance also requires new technical capacity, improved data sharing and political support.7
Building an international tax unit to participate in international tax data exchange: Recent reforms to international tax rules call on all countries to voluntarily share information with home countries about accounts held overseas by their residents. However, significant investments are needed in order to participate. Countries need to be able to receive, ensure the security of and use international information. And they need to be able and willing to share data reciprocally. A small number of lower-income countries have begun putting in place that infrastructure. However, progress has been slower than hoped and actual revenue gains so far very limited amidst challenges in meeting minimum standards for participation and difficulties in successfully using new information and enforcing compliance.8
Strengthening audit and enforcement capacity: Special investment may be made in recruiting and retaining audit and enforcement capacity through expanded staffing, higher recruitment or other retention strategies.
Investing in digitalization of tax administration: Digitalization can play a key role in improving data sharing, identification of under-reporting and audit selection. The government could focus, in particular, on strengthening data sharing with key public and private actors and on improving identification of high-risk cases for audit. This would build upon initial digitalization undertaken in recent years.
Strengthening property mapping, identification and valuation: New investments in property mapping, identification and valuation could contribute to (a) improved collection of property taxes, (b) improved identification and collection of rental income taxes and (c) improved ability to identify high net worth taxpayers via improved information about property wealth. This would only target one category of wealth, and related income, but recent reform success in other low-income countries points toward the potential for significant improvements in outcomes.9
Reviewing existing tax incentives and exemptions: Many countries in the region have recently reviewed their incentive regimes and made efforts to (a) ensure that the Ministry of Finance approves all incentives, (b) ensure that all incentives are documented in legislation, and (c) introduce annual published assessments of the revenue impact of incentives, by firm. In many countries this has led to greater coherence and monitoring, and the elimination of poorly designed or monitored incentives.
Study the potential for a new wealth tax: In response to growing international interest, the country could launch a study of the potential of introducing a wealth tax. In favor of a new tax, your advisors note that your country faces very high levels of inequality, with a number of large intergenerational families controlling significant parts of the economy. However, they note that (a) collecting a wealth tax in practice could be difficult given limited data about assets, and concerns about wealth being moved offshore, and (b) that there may be other more immediate and simpler opportunities for improving collection from wealthy individuals.
Building popular support: Given the likelihood of resistance from elite taxpayers, and their supporters, the government could seek to build a popular base of support for reform. One question surrounds framing: should these efforts be presented as a progressive effort to tax the rich, as an effort to ensure that everyone pays their fair share under the law, or something else? A second question is what measures the government can take to build public confidence that new revenues will be used effectively, including options like increased budgetary transparency, explicit new spending initiatives or earmarking of new revenues.
Addressing collusion and political interference: Alongside these specific recommendations your advisors note that because existing weaknesses have been significantly driven by collusion/corruption and political interference the success of any strategy is likely to depend on developing a strategy to address those broader challenges.
Guiding Questions
You have decided to establish two working groups, each of which you will lead, to discuss next steps in reform planning. Their mandates are as follows:
Broad Strategy: Given limited capacity, which options among those proposed by your advisors should be prioritized first – and what should be key elements of the strategy for making those initiatives successful?
Digitalization Strategy: The government has already committed to – and has international support for – further investing in digitalization in order to improve data sharing, identification of underreporting and audit selection. Given that the technology itself is already in place, what will be the key elements of your strategy to ensure that those key functions are improved in practice?
6 Data derived from an actual survey conducted with taxpayers in Sierra Leone in 2020 and 2021 (van den Boogaard, Orgeira and Prichard 2023). The share of respondents who indicated that revenue for recovery should come from more taxes on the richest was 55% prior to the pandemic, and 83% at the end of the pandemic. By contrast, support for broad based taxes rose from 24% to 35%, while for large businesses support rose from 41% to 72%. When taxpayers were limited to selecting one revenue source to prioritize 27% selected taxes on the rich, 33% selected taxes on large businesses and only 10% selected broad based taxes.
In June 2010, Benigno Aquino, a chain smoker, was elected President of the Philippines. President Aquino campaigned on a 16‑point agenda for reform, which he called his “Social Contract with the Filipino People.”1 This social contract promised to transform health from “just another area of political patronage” to a “measure of good governance.” President Aquino also committed not to increase and reduce, where possible, taxation and tariffs impacting regular citizens. When he took office, Aquino was alarmed to learn that an estimated 30% of Filipinos died prematurely due to inadequate access to health care. Hence, the President appointed renowned surgeon Dr. Enrique Ona, Health Secretary, with the specific charge of alleviating the burden of disease in the Philippines by expanding the national health insurance program (PhilHealth) to all Filipinos.
Tobacco use was a major cause of morbidity and premature mortality in the Philippines. Historically, the Philippines has had one of the highest rates of smoking in the world. Low taxes on tobacco products made cigarette prices in the country among the lowest in the world. In 2007, more than a quarter of 13-15-year-olds were regular smokers,2 and in 2008, more than half of men (53.2%) and 12.5% of women aged 20 or older smoked.3
To address tobacco-related deaths, in 2003, the WHO established the WHO Framework Convention on Tobacco Control (FCTC) with the goal of reducing smoking worldwide, including by promoting higher taxation on tobacco products.4 The WHO FCTC was based on substantial research over many years demonstrating the effectiveness of higher tobacco taxes and prices in reducing the consumption of cigarettes and other tobacco products.5-7
The Philippines joined 167 other WHO Parties (member states) in signing the WHO FCTC in 2005.8 Nonetheless, tobacco cultivation has also traditionally been a source of income for many Filipinos in the tobacco-producing provinces of the country, where multiple farmers planted tobacco in addition to other profitable crops.9 In 2010, tobacco excise revenues accounted for 0.3% of the Philippines’ GDP.10 In 2010, tobacco farming accounted for 0.4% of total agricultural employment, and farmers produced more than 70 million kilograms of tobacco leaf valued at PhP 4.85 billion (USD 108.4 million)11, and approximately 40 million kilograms were exported.12
Funding Expanded Universal Health Coverage
As Health Secretary, Dr. Enrique Ona had the mandate to reduce the burden of disease in the Philippines by expanding the national health insurance program (PhilHealth) to all Filipinos. However, given President Aquino’s promise not to introduce new tax measures, Secretary Ona recognized that to fund the increase in PhilHealth coverage, he would have to leverage existing government revenue streams.
Secretary Ona was appointed at the beginning of President Aquino’s presidency, and the Framework Convention on Tobacco Control Alliance, Philippines (FCAP) knew that with this new administration in office, a new legislative session would convene, and there would be new leadership in the Department of Finance (DoF) and Department of Budget and Management (DBM). This meant that many policies, including the tobacco and alcohol taxes, would likely be reviewed.
Therefore, the FCAP requested a meeting with Secretary Ona to advocate that the Department of Health (DoH) support dramatic Sin Tax Reform to fund the cost of extending PhilHealth coverage to all citizens. Based on his experience as a doctor who had seen many patients with tobacco-related diseases over the years, Dr. Ona agreed to work for an increase in taxes on tobacco products, though he was unsure how best to design the tax policy to ensure sufficient revenue. He was also not sure how to muster political support and counter the forceful political influence of tobacco growers and cigarette manufacturers.
After their meeting with Secretary Ona, FCAP invited Action for Economic Reforms, a Philippine NGO experienced in advocacy and economic policy research, to collaborate on promoting the Sin Tax Reform. “We had a new President, so there was a breath of fresh air—the possibilities seemed endless,” one advocate reflected. “It was an opportune time for groups to re-strategize the approach to passing sin tax reforms.”
Action for Economic Reforms received a grant from the US-based foundation Bloomberg Philanthropies to unite local and national tobacco control, health care, and economic reform groups. They called their collaboration ‘the sintax coalition’. Representatives from the groups met to establish a shared goal: to improve public health by reducing smoking and, secondarily, to generate revenues for health by raising taxes on cigarettes and alcohol.
Despite being a smoker himself, President Aquino supported the idea of raising taxes on tobacco products to discourage smoking and raise revenues to expand healthcare access. He agreed after being convinced by his advisers that it did not violate his campaign promise of “no new taxes” as this was just a restructuring of existing taxes. In August 2011, he announced his official legislative agenda, which included increasing ‘sin taxes’ to fund the expansion of universal health coverage. He directed all his cabinet secretaries to join Secretary Ona in prioritizing Sin Tax legislation reform.
Civil society coalition members set up meetings with legislators allied with the Aquino administration to ask if they would “champion” a Sin Tax Reform measure. They focused initially on members of the Ways and Means Committee in the House of Representatives, where tax bills were filed first and where legislators with known connections to the tobacco industry typically dominated the Committee.
Proponents and Opponents of the Sin Tax Reform
One key strategy used by reform proponents involved presenting the Sin Tax not as a tool for generating revenue but rather as a health-focused instrument that would help attain Universal Health Care. A government official explained:
“But when we said, ‘This is really a health measure, not a revenue measure,’ I mean, then you are able to create more allies, yeah? Because health resonates with more people than—I mean, if you say, ‘Revenue,’ people just said, ‘You’re just greedy, you want more money for government to corrupt.’”13
Proponents included civil society organizations, international organizations, and government departments and offices such as the Office of the President, the Department of Budget and Management, the Department of Finance, the Bureau of Internal Revenue, the Department of Health, some legislators, and local government executives. Moreover, “political mapping was also undertaken continuously throughout the legislative process to identify supporters, fence-sitters and staunch opponents.”13
Proponents anticipated strong opposition from opponents such as the National Tobacco Administration, the Philippines Tobacco Institute, the Philippines Tobacco Growers Association, as well as some legislators who were part of the Northern Alliance, an influential group composed of members of Congress from Northern Luzon.
Hence, before speaking publicly about the Sin Tax Reform, Secretary Ona, DoF Secretary Cesar Purisima, and DBM Secretary Florencio Abad met to align their messaging. The DoF convened meetings, inviting point persons from other government agencies and civil society to share updates and concerns and to coordinate actions in support of the Reform. Undersecretary of Finance Jeremias Paul emphasized the value of a “whole of government approach,” noting that “If we’re not united, powerful opposing lobbies will capitalize on that.”
The core group of proponents met regularly in what they called the “war room” to align strategies, share their perspectives, and have a unified response to issues raised by the tobacco industry and their allies. They also allowed members to enact their own strategies if they were geared towards a common goal. They also anticipated that the issue of burden sharing between the tobacco and alcohol industries would most likely be an issue raised in Congress. Discussions ensued, and consensus was reached that they needed to choose their battles. In the case of tobacco versus alcohol, they focused on tobacco.13In the case of alcohol, the government’s key objective was to be compliant with WTO rules. The Philippines lost a case in the WTO as it was deemed that domestic alcohol products had a favorable tax treatment over imported ones. Moreover, tobacco use posed a bigger health challenge than alcohol at that time. As an NGO actor explained:
“The alcohol people threatened not to support the reform unless they were given some concession. So we didn’t fight that battle, in order to get the tobacco reforms”13
To be consistent with existing Sin Tax legislation and mitigate opposition, proponents also proposed allocating a portion of incremental revenues to encourage farmers in tobacco-growing provinces to shift to other crops or economic activities. Secretary Ona consulted with the Department of Agriculture’s National Tobacco Administration to understand how the Reform might impact tobacco farmers and cigarette manufacturing workers. Because of this, some were concerned Dr. Ona might favor more conservative tax increases. He countered, “I was aware that five of our provinces depend on tobacco as a major industry,” Ona explained. “I wanted to ask them what their concerns were and to convince them that this was a health issue.”
Data Proves Critical
The tobacco industry and their allies raised a lot of issues about the wisdom of raising tobacco taxes significantly. They claimed that raising tobacco taxes increases smuggling and illicit trade, is anti-poor or regressive, that revenues will go down, and it will have a negative impact on employment. The alcohol industry was not vocal in its opposition.
To counter tobacco industry lobbying, civil society groups reached out to local chronic disease experts to estimate the economic costs of smoking and compare it to the tobacco revenues collected by the government. Dr. Antonio Dans, a Filipino epidemiologist, had been studying the economic and health costs of tobacco for more than a decade. His work had never been used for advocacy. One advocate explained:
“It had worked for the tobacco industry that nobody could connect these things. All of these data existed, so the work in 2011 was to connect the dots.”
Dr. Dans updated his previous studies using current data and found the cost of death and disease resulting from four tobacco-related illnesses (lung cancer, chronic obstructive pulmonary disease, coronary artery disease, and cerebrovascular disease) to be PhP 188.8 billion (USD 4.22 billion) — nearly 2% of GDP.14 Costs included health care, productivity losses, and premature death losses.
Dr. Dans also modeled how many premature deaths could be prevented given various combinations of price elasticity of demand values and excise tax increase assumptions. He created a table showing how various combinations of price elasticity of demand and magnitude of tax increase assumptions would affect smoking prevalence and revenue generation. The exercise was meant to point out that regardless of the price elasticity of demand assumption, the net impact on revenues would be positive. Drawing on the data, the DoF and coalition members decided to advocate for the highest tax rate possible. Traditionally, DoF and DBM preferred not to earmark legislation because it restricted the government’s flexibility. In this case, all government parties agreed that it will be an exception and that the incremental revenues from higher tobacco and alcohol taxes would be “soft-earmarked” with the DoF drafting the implementing regulations.
The DoF calculated the price elasticity of demand for cigarettes to be –0.5, meaning that a 10% increase in cigarette prices would yield, on average, a 5% reduction in cigarette consumption. Tobacco industry stakeholders argued that elasticity was closer to –0.8, suggesting that a tax increase would discourage smoking so much that the revenue-generating goals of the bill would be undermined. Lower consumption would have a negative economic impact, they warned, stifling business for local tobacco farmers and cigarette manufacturing companies. Some also cautioned that such a tax increase would disproportionately burden poor Filipinos.
In contrast, proponents of the tax increase cited studies showing that job and economic losses owing to higher tobacco taxes were usually more than offset by increased spending and employment in other sectors. Studies suggested money previously spent on tobacco was diverted to other goods and services.15,16 In response to arguments that higher tobacco taxes would be regressive, the DoF countered that poor Filipinos had the most to gain because they would not otherwise be able to afford health care.
Traditionally, the DoF took the lead on submitting tax proposals to Congress. For the Sin Tax legislation, Paul reflected, “What differentiated this from past efforts was that health and finance were working together.” Ona and Purisima entrusted day-to-day coordination and communications to their under-secretaries. DoF Undersecretary Paul and his team helped Secretary Ona determine how much revenue the DoH required to achieve its goals of universal health coverage, while DoH Undersecretary Herbosa worked with the DoF and civil society coalition to emphasize the legislation’s health objectives.
Getting the Law Passed
With respect to the tax reform, an agreement was also reached with President Aquino on the negotiable and non-negotiable parameters so that discussions with the industry stakeholders would be transparent. The non-negotiable reform parameters were: (a) removal of the price/brand classification freeze, which gave legacy brands a tax advantage over new entrants; (b) indexation of tax rates to inflation; and (c) compliance to WTO rules with respect to alcohol. The negotiables were: (a) length of transition period from a four-tiered structure to a two-tiered or unitary tax structure; (b) rate of tax increases; and (c) period of time between tax rate increases.
Legislative power in the Philippines rests with Congress, which is made up of the House of Representatives and the Senate. The House, which has 250 members, and the Senate, which has 24 senators, are important for enacting tax legislation such as the Sin Tax. Under the Philippine Constitution, all revenue bills must emanate from the House of Representatives. The Senate has the power and responsibility to suggest changes or modifications to proposed Bills.13
Historically, proponents had typically faced opposition in the Ways and Means Committee of the House, which was the first step in getting a revenue bill passed, and almost always, this Committee was dominated by the tobacco industry. Fortunately, the 2010 House elections elected a new chair of the House Ways and Means Committee who did not have ties with the tobacco industry.13
Even before the Sin Tax House Bill was published, the tobacco industry mobilized farmers and factory workers to protest with the aim of stopping or at least slowing the passage of the House Bill. Northern Alliance members proposed lower rates and a three-tiered tax structure. Faced with this political pressure, the House Bill’s authors made some compromises, agreeing to a two-tiered structure and a phased transition. San Miguel Corporation, one of the largest corporations in the Philippines and the dominant beer player, with revenues equivalent to 5.4% of GDP, was a critical player in advancing this Bill. To secure their support, pro-Sin Tax legislators lowered the premium on fermented liquor brands to include its popular premium beer brand. Similar negotiations were made with representatives of the Distilled Spirits Association of the Philippines.
Despite organized opposition from the tobacco growers and manufacturers, the Filipino public, recognizing the potential health care benefits, was overwhelmingly supportive. An organization representing local government leaders appealed to a nationally known former governor from a tobacco-growing province to endorse the legislation by publicly denouncing the notion that higher Sin Taxes would lead to the demise of the Philippines’ tobacco industry—a popular argument among opponents. The Governor supported the local government leaders and argued the tax would “level the playing field” for smaller domestic companies trying to compete with Philip Morris Fortune Tobacco Corporation (PMFTC), a joint venture between Fortune Tobacco Corporation and Philip Morris International. Secretary Ona believed the former Governor’s public support of the Bill convinced several politicians from northern tobacco-producing provinces to support it.
The coalition organized press conferences, testified before Congress, and worked closely with media outlets to broadcast data on the negative effects of smoking. Former Secretaries of Finance and Health who had participated in past Sin Tax Reform efforts spoke publicly in favor of the Bill. When Secretary Ona spoke publicly, he emphasized the Bill’s health aims. He noted:
“…[This] was probably the most important role I played: to make it very clear to everybody to forget about it being a tax measure and focus instead on it being a health measure.”
Dr. Dans and other coalition members presented the data showing how different tax rates would impact smoking and revenue generation during legislative hearings. Proponents began calling the Sin Tax Reform Bill an “anti-cancer tax” and rallied more than 50 medical associations to sign a petition in favor of it.
A government official observed, “Anything coming from government is considered propaganda, and anything coming from legislators and other politicians is perceived as meant to enhance their political careers.” To put additional pressure on Congress, the coalition created a public webpage that tracked which legislators supported the bill and which opposed it. “Elections were scheduled for May 2013, and people were checking how senators had voted,” one advocate explained. “We made it an election issue.”
International credit rating agencies were also watching the Bill’s trajectory carefully. They recognized its potential to broaden the Philippines’ fiscal base for higher spending on infrastructure, health, and education. In October 2013, Moody’s Investors Service joined Fitch Ratings and Standard & Poor’s Ratings Services in upgrading its assessment of the country’s debt quality to a level below investment grade. The DoF hoped to achieve an investment grade rating—which would reduce some borrowing costs and attract more investment funds—by 2014.
The Sin Tax Bill, being a revenue bill, required House passage, and Congressman Sid Ungab, Chairman of the Ways and Means in the House of Representatives had to strategize how to get the bill out of the committee, mindful that a majority of members were allied with the tobacco industry. To address this hurdle, Secretary Purisima requested a meeting with the President, the House Speaker, and key members of the Ways and Means Committee, on the reform parameters.
They compromised on the House version, knowing they could work on a better Senate version, and it passed on June 6, 2012.13
After the House approval, the Sin Tax House Bill required Senate passage. The Senate could either propose its own version of the Sin Tax Bill or just ratify the House bill version. However, Senator Ralph Recto, then chairman of the Ways and Means Committee, filed a Senate version of the Sin Tax Bill which, when passed, was very similar to Philip Morris’ low-rate proposal. Consequently, there was an outcry from civil society, with some coining the Senate bill as the “Recto-Morris Bill”. Sin Tax proponents in the Philippines used various strategies, including lobbying, media advocacy, and daily rallies asking for Senator Recto’s resignation. Under public pressure, Senator Recto resigned from his position as Chairman and was replaced by Senator Franklin Drilon, whose wife died of lung cancer. A government official explained:
“But what really moved the reform for us was that the chairman, [he] was behind us all the way. So, he used his powers and authority as the Chair to move the discussion and the approval in favor of the reform.”13
The Senate version of the bill proposed by Senator Drilon had a unitary tax structure, tax rates indexed to inflation, and a five-year transition period.
The House and Senate passed separate versions of the measure; the difference between the two Bills was subsequently resolved in a Bicameral Conference Committee. This was another challenge as the tobacco and alcohol industries were able to put in their allies in the Bicameral Conference Committee. Both Senator Drilon and Congressman Ungab, while chairing the Senate and House negotiating panels, respectively, did not have full control of the membership of the Bicameral Conference Committee as it was the Speaker of the House and the Senate President (a known tobacco industry ally) who would finally make that determination. After long deliberations, consensus was reached in the Bicameral Conference Committee, and their version of the Bill had to be ratified by both Houses of Congress.
On December 11, 2012, the committee signed the report and sent the measure to the President for approval. Both Houses of Congress ratified the bicameral version of the Sin Tax Bill with a very narrow margin in the Senate – 10 votes for and 9 votes against. President Aquino signed the Bill (Republic Act 10351, more commonly referred to as “the Sin Tax Reform Act”) into law on December 19, 2012, with the higher tax rates taking effect on January 1, 2013.
Initial Results
With the passage of the Sin Tax Reform Law, cigarette taxes increased by up to 340% in the first year of implementation18, and the average price per cigarette pack increased from PhP 21.12 in 2012 to PhP 31.26 in 2013.19 Total Sin Tax revenue collections for tobacco and alcohol reached PhP 70.4 billion (US$1.57 billion) and PhP 33 billion (US$737.7 million), respectively during 2013. The total tobacco excise tax collection in 2013 represented a 114% increase over 2012 collections, while total alcohol tax collections grew by 38%. The Sin Tax Reform Act resulted in an unprecedented year-over-year increase in the DOH’s budget of 57%. 85% of incremental tobacco tax revenues and 100% of incremental alcohol tax revenues were earmarked for health. Of these combined revenues, 80% would be used to finance PhilHealth, the attainment of the Millennium Development Goals, and health awareness programs. The remaining 20% would be used for health infrastructure improvements and support for indigent patients. Incremental tobacco tax revenues not supporting health (15%) would fund economic development projects in tobacco-growing provinces.
Surveys conducted in 2014 found a marked decline in smoking across all demographics. The most dramatic declines were in the lowest income quintile (from 38% to 25%) and among adults 18–24 years of age (from 35% to 18%). Proponents of the Sin Tax believed the reduction in smoking was largely the result of fewer Filipinos starting the habit. Dr. Antonia Dans, who had presented the costs of tobacco-related diseases during the Sin Tax Reform debates and whose epidemiologic research spanned a variety of lifestyle-related diseases, attributed the change to the Sin Tax Reform effort. He said:
“Studies show that people don’t exercise in the Philippines because there are no facilities for nonmotorized traffic. There’s no place to walk or to bike. Filipinos don’t eat vegetables because they’re too expensive, and they smoke because tobacco is so cheap. So, we used this logic, and whereas for 30 years we were unable to reduce smoking by telling people it was bad for them, with just a small tax measure, the prevalence went down from 31% to less than 26%. This seems small, but it’s the equivalent of 3 million fewer smokers in 2013. Our estimate is that about 32,000 premature deaths were averted.”
Philippine Statistics Authority. A Filipino family earns an average annual income of P206 thousand in 2009 (preliminary results from the 2009 Family Income and Expenditure Survey). 2010. https://psa.gov.ph/statistics/incomeexpenditure/fies/node/1405
Steele G, Avila J, Miller D, Britan G. Ending extreme poverty in the Philippines through urban‑led growth. In: Shah R, Unger N, eds. Frontier in Development 2014: Ending Extreme Poverty. Vol Washington: U.S. Agency for International Development; 2014:82‑87. https://seatca.org/dmdocuments/Media_Farming%20Regional%20Paper_final.pdf
Over several decades, Nigeria has confronted major health crises characterized by a double burden of disease — preventable infectious diseases and a rising prevalence of non-communicable diseases (Li et al., 2022). Vaccine-preventable diseases, in particular, have contributed to the country’s high child and maternal mortality rates (Ophori et al., 2014).
Minister Muhammad Ali Pate was appointed Nigeria’s Minister of State for Health in June 2011. Before he was appointed Minister of Health, he served as the Chief Executive Officer of the National Primary Healthcare Development Agency (NPHCDA) for three years, made significant progress in improving Nigeria’s primary healthcare system, and initiated crucial health sector reforms during his tenure.
President Goodluck Jonathan appointed Dr. Pate Minister of Health to continue his previous work at NPHCDA. His mandate included improving efforts to eradicate polio and enhancing routine immunization. Initially focusing on polio, his goal as Minister of Health expanded to encompass child and maternal health through the Saving One Million Lives campaign. The Saving One Million Lives campaign by Minister Pate was developed to ensure that efforts to improve health in Nigeria also addressed other urgent health issues such as measles and malaria.
This case study explores how Minister Pate was able to navigate the fraught politics of Nigeria and win the support of the President, key Cabinet allies, and 36 state governors for a country-wide transformative health initiative.
Building a Guiding Coalition
When Minister Pate took office, there were rumblings of discontent regarding Nigeria’s health system, but health issues were not high on the national political agenda. Plus, given the decentralized nature of the health system, the Minister had limited control over how each of the 36 states spent their federal budget allocation. Although a significant part of the state budget came through federal allocations by a constitutionally determined formula, the fiscally decentralized federal system of government allowed states fiscal autonomy. The result was limited federal oversight or accountability regarding how much states allocated to health and how such resources were allocated. National Health Account data showed that most health resources were spent on politically popular curative facilities. These were often geared to the health needs of wealthy citizens. Even though the federal government had conceptually sound health policies, execution and enforcement at the state level were difficult.
Developing a Legacy Goal
Soon after taking office, Minister Pate assembled a core leadership team, led by a long-time trusted colleague, Dr. Kelechi Ohiri. With the support of his core team, Minister Pate reflected on the healthcare landscape in Nigeria to determine what he wanted to accomplish during his limited term of a maximum of four years. He said:
“I built a very strong team, including some I had mentored before, like Dr. Kelechi Ohiri. I chose people who were not only competent but had the right mindset and character attributes to help me deliver on our goals. As a Minister, very early on, you need to know what you want to accomplish. Build a good team, mobilize resources, and ensure everyone is accountable, including yourself. Focus on execution, or you will not achieve much.”
Minister Pate wanted to focus his agenda on something that would help Nigeria achieve something tangible, particularly given the multiplicity of problems within his main portfolio of primary healthcare. As he reflected, he realized that all around him was a culture of input-based thinking. Healthcare policy was made based on what else could be put ‘in’ to the health system. He wanted to shift the conversation to what was coming ‘out’ of the system, i.e., an outcomes-based approach. To drive this mindset, Minister Pate asked his ministry:
“What are we here for?”
When they thought about primary healthcare, saving lives was the most concrete outcome. The next step was to define ‘saving lives’ in a way that was easy to communicate. From this discussion, Minister Pate’s signature program, “Saving One Million Lives (SOML),” was born.
SOML was an aspirational target that was big enough but also tangible enough to focus people on the outcomes that matter and to work backward toward the inputs. SOML aimed to strengthen primary healthcare and prioritize interventions that could save lives, such as improving maternal and child health, eliminating mother-to-child transmission of HIV, strengthening immunization, scaling up access to essential medicines, controlling malaria, and improving child nutrition.
SOML built on existing policies outlined by the National Strategic Health Development Plan and the President’s Transformation Agenda rather than introducing new ones by way of strengthening existing delivery channels.
Minister Pate also used the Lives Saved (LiST) tool to prioritize the critical intervention areas that would contribute the most to lives saved. Based on this analysis, the six key priorities of SOML were improving maternal and newborn child health, eliminating mother-to-child transmission of HIV, strengthening routine immunization and achieving polio eradication, scaling up access to essential medicines, malaria control, and improving child nutrition. The underlying idea was that to save one million lives; the primary healthcare system would have to be strengthened by increasing health personnel, introducing performance management systems to increase health worker productivity, improving quality of care, and using information and communication technology for the supply chain management. By linking health systems strengthening to concrete outcomes, Minister Pate hoped that beyond saving one million lives, the benefits of these systemic changes would continue. Nonetheless, Dr. Pate realized that SOML’s success depended on the political will that supported it. This began with the President.
Working with the President
According to Minister Pate:
“When I started in 2008 as CEO of the Primary Healthcare Development Agency, it was polio that led the previous President to appoint me. To deal with polio and immunization, I had to build a primary healthcare system. By 2011, when the new President was elected, he asked me to join his government to build on the work I had started.”
Soon after his appointment as Minister of Health, Dr. Pate made sure to meet with President Goodluck Jonathan to thank him for the honor of appointing him to serve. In that meeting, he promised to serve the President with his very best and asked him for one thing in return:
“If I make any mistakes or if I am not doing something you really want, I want you to call me directly. And if I have a similar issue with you, I want to be able to come to you directly.”
This conversation formed the foundation for an effective working relationship and proved useful for the duration of Pate’s term.
To communicate SOML to the President, Minister Pate recollected what he knew about the President. Two key factors proved important. Firstly, President Jonathan had lost several siblings to preventable diseases at a very young age. Secondly, President Goodluck’s term had begun with a deeply unpopular move – the cancellation of longstanding subsidies to Nigerians on oil and petroleum gas.
Saving children from death and disease was something the President had a connection to, and the public was concerned about it, so it made for a compelling goal.
After the President’s support for the SOML campaign, Minister Pate provided monthly written updates to the President to regularly reinvigorate his political will and to maintain their connection. The President wanted to say that he had eradicated polio and ‘saved one million lives’ as part of his Transformation Agenda. His and Minister Pate’s legacies were aligned. Minister Pate said:
“Polio and immunization were embedded within the context of primary healthcare revitalization. We reframed the polio fight to include vaccines and saving the lives of children and mothers, rather than isolating it as a separate issue.”
Minister Pate gained this high-level backing by aligning SOML with the President’s personal experiences and the public’s needs.
Finance Minister
After the President, Minister Pate set his sights on bringing the Minister of Finance, Ngozi Okonjo-Iweala, on board with SOML. He knew Minister Okonjo-Iweala as a senior colleague from their time together at the World Bank, where she remained until her cabinet appointment. He had built on this pre-existing relationship with her by visiting her in Washington, DC, after her appointment but before her taking office. He also knew that during her previous tenure as Minister of Finance, she had been frustrated with the health sector because she did not have a clear sense of what had been accomplished with the funds she had allocated.
To get Okonjo-Iweala on board, Minister Pate had to stress the outcomes-based approach to SOML. Okonjo-Iweala was swayed by SOML’s clear definition of goals and deliverables because she could easily see and understand it as Minister of Finance. Thus, she was willing to support it. She asked Minister Pate to serve on the Economic Management Team and the Economic Management Implementation Team – two intersectoral working groups housed within her ministry. This was the first time the health sector was fully represented in such a body.
As part of the Minister of Finance’s Economic Management Team, Minister Pate gained a higher-level understanding of government priorities and connected with his colleagues on the team – including the Minister of Planning, the Director General of the Budget Office, and the Chief Economic Advisor to the President. He made SOML one of the key deliverables of the Economic Management Team, which further solidified their buy-in to its success.
Consequently, Minister Pate convinced both the President and the Minister of Finance to invest part of the money recouped from the cancellation of oil subsidies in maternal and child health to deliver results for the public. In September 2011, with President Jonathan’s and Minister Okonjo-Iweala’s support, Dr. Pate made a public announcement about defining his term with the goal of Saving One Million Lives in Nigeria.
Managing Stakeholders with Influence
With the support of the President, the Minister of Finance, and high-level officials from the Ministry of Health, Minister Pate moved to identify other key stakeholders that needed to be managed. Later in his career, he would learn more about using stakeholder analysis to explicitly map supporters and opponents against their level of influence. Still, at this time, he took a more intuitive approach. He maintained an internal inventory of the relationships he had cultivated and leveraged his social networks to forge connections with those who were truly influential, regardless of their positional authority.
Within his own ministry, Minister Pate had traditional authority by virtue of his position as Minister of State for Health, but this was supplemented by good relationships with the Federal Minister of Health (whose primary focus was on tertiary care and health insurance, among other areas), the Permanent Secretary, key directors, and the Primary Health Care Agency.
Nonetheless, within his own health ministry, Minister Pate sensed a feeling of “passive resistance.” The Health Ministry had traditionally taken responsibility only for the allocation of the federal health budget to states without monitoring the use of the state health budgets, with minimal state accountability and little regard for impact. At the outset, senior officials in the health ministry thought they could ignore Minister Pate’s SOML initiatives and “let it die on its own.” Nonetheless, Minister Pate persisted onwards with the higher-level health officials who formed his guiding coalition to prove to these opponents that SOML was not going away.
As SOML gained traction in the form of support from the President, the Finance Minister, and more state entities, and by raising substantial funds, the naysayers not only came on board but also began to be champions of the initiative.
As Minister Pate continued to work to achieve his mandate, he had a secret weapon on his side: the initiative’s name – “Saving One Million Lives.” By framing the program this way, opposing stakeholders, particularly those in the political sphere, had a challenging time voicing their opposition to “Saving One Million Lives.”
Engaging Governors and Community Leaders
Minister Pate leveraged his previous relationships with governors and community leaders to understand the importance of state-level cooperation, especially when it came to vaccinating citizens. He organized forums and secured commitments from state governors to support primary healthcare improvements. Additionally, he established the Northern Traditional Leaders Committee on Primary Healthcare to engage trusted community leaders in vaccination and health campaigns. He explained:
“When it came to vaccination hesitancy, we worked to earn the trust of communities and community leaders. We created the Northern Traditional Leaders Committee on Primary Healthcare, which engaged religious and community leaders across Northern Nigeria. This network became crucial in planning and implementing vaccination campaigns. To select the Northern Traditional Leaders, we went to the Sultan and asked him to convene a group of representatives from each of the 19 states in the North. The Sultan and a committee selected leaders who were relatively younger, stronger, respected, and trusted. We then organized them into a committee and enabled them to act effectively. To engage communities, we provided them with information and involved them in planning, which built legitimacy in the eyes of the people.”
As he had anticipated, Nigeria’s 36 state governors were key stakeholders whose support Minister Pate needed to save one million lives. Fortunately, Minister Pate had existing relationships with several governors and with the Director General of Nigeria’s Governors’ Forum. The Governors’ Forum had preexisting goals to eradicate polio and implement effective routine immunization programs as part of Nigeria’s 2009 Abuja Commitments to Polio Eradication. Minister Pate said:
“When I became Minister, it was easier for me to build on the relationships I had already established with the governors. As CEO of the Primary Healthcare Development Agency, I had worked closely with the Governor’s Forum, helping to organize their secretariat and getting them to sign the Abuja Commitment Declaration in 2009. This previous work allowed me to leverage those relationships when I became Minister.”
While this was helpful in aligning them with SOML, convincing them to relinquish their budget autonomy was still a challenge. Ultimately, the President had to play a significant role in bringing the governors on board.
The President asked the Governors to be accountable for progress in their states. Minister Pate’s team provided each state with a ‘Countdown to 2015’ one-page document summarizing how many lives the state could save by expanding specific services relevant to its context. This provided each state with its own baseline and endline target.
Once the states had pledged their commitment to their targets, Minister Pate’s team set up a scorecard system tracking progress state-by-state. The data comparing state performance was presented at the quarterly meeting of the Presidential Task Force on polio eradication, with the governors in attendance, presided over by the President, and quickly became a major incentive for the states to improve performance. Initially, some governors were uncomfortable with the pressure to be accountable and pushed back. However, according to Minister Pate, the measurement of performance became:
“An inflection point shifting the dialogue to focus on the data to its use in decision-making and results.”
Furthermore, the scorecards on state performance were published in newspapers. This decision was made to ensure that data collected from the public was ‘given back’ to the public and to further motivate state progress.
Finally, there were donors. Minister Pate needed donor support to generate more innovative ideas for technical assistance and strategy for the maternal and child health programs associated with SOML. Traditional and particularly non-traditional donors were eager to fund the initiative, and he was able to work with philanthropic foundations with flexible sources of funding to recruit world-class experts to help with ideation and design. He explained:
“As Minister, I was very active in mobilizing resources. I leveraged traditional domestic financing, multinational financing, and other sources to move the agenda quickly. We raised resources through innovative financing, which helped draw states in the direction we wanted.”
Implementing Strategically
As he worked to bring stakeholders on board, Minister Pate was invited to attend the Harvard Ministerial Leadership Forum in June 2012. This gave him the opportunity to learn about tactics for effective policy implementation and organization. In his own words:
“I was internally strengthening my hand while externally learning and strengthening relationships to succeed.”
The President officially launched SOML in Nigeria on October 16, 2012. The idea behind this campaign was a national rallying cry to end preventable infectious diseases and curtail infant and early childhood mortality. SOML had a strong brand identity (including a logo) and a deliberate communications strategy.
Minister Pate created a culture of collaboration and a sense of obligation amongst public and private sectors to do their part by positioning the campaign as a collective social movement across the nation. The communications strategy allowed key actors to pledge how many lives they would save – the private sector initially pledged to save 30,000, which later increased. Finally, and perhaps most importantly, SOML’s multichannel messaging plan created a sense of accountability to the people. This made it more difficult for state governments to allocate resources away from the program’s initiatives.
Once launched, Dr. Pate had to ensure implementation success. He needed some control over state-level health spending to ensure compliance with the national goals.
To this end, he introduced three key nationally managed elements to the program. The first was developing a robust data management system to monitor and evaluate performance. Historically, data had been collected independently at the state level, but in order to improve its reliability and comparability across states, he implemented a centralized data management system to enable the tracking of outcomes for the nationally outlined priorities. Furthermore, this data would be used for decision-making purposes regarding future state health budget allocations.
The second element was stewardship and stakeholder engagement. It involved introducing a steering committee housed within his ministry comprising representatives from federal and state government, professional associations, civil society associations, and donor groups. The goal of this committee was to enhance coordination through increased transparency and mutual accountability for the outcomes determined by the data collection. Pate chaired meetings with the steering committee every three months to review progress and ensure stakeholder alignment.
The final element introduced by Minister Pate was a program delivery unit, jointly accountable to the health and finance ministries, to support execution and ensure effective, high-quality delivery. This was led by competent professionals with a focus on results.
After Strategic Implementation
Minister Pate resigned in July 2013, confident that SOML was institutionally secure and embraced by his successors. By 2018, one million lives had been saved, and SOML had raised over US$1 billion in investments. The initiative had survived three Ministers of Health and fundamentally shifted the mindset towards primary healthcare. SOML’s principles were further institutionalized through a partnership with the World Bank, rewarding federal and state governments based on performance.
Looking back, Minister Pate was gratified by the adoption of outcomes-based thinking within the ministry and state governments. However, he reflects on areas for improvement, such as spending more time with state governors, consolidating information management systems, focusing on public sector supply chains, and integrating health insurance into SOML plans. His final reflection underscores the importance of strategic decision-making in complex systems:
“In a complex system, you cannot always fight in all directions. You have to choose which battles to fight and when.”
In 2020, “Nigeria was declared free of wild polio in 2020” (The WHO, 2023).
2023 Reappointment
In 2023, Minister Pate was again appointed Coordinating Minister of Health & Social Welfare, Federal Republic of Nigeria. He said:
“I’m refreshing and learning from every experience I have had. When I enter a new role, I treat it as a fresh start and apply the lessons learned from previous experiences, ensuring we build strong teams, mobilize resources, and maintain a clear focus on execution. In my current role, I quickly did a stock take together with my colleague the Honorable Minister of State, engaged with the ministry bureaucracy and agencies, and developed an agenda and blueprint. We are focused on saving lives, reducing pain, and producing health for all Nigerians. I brought in capable hands, the best I could find, to ensure we could deliver on our objectives.”
References
Li, Z., Shi, J., Li, N., Wang, M., Jin, Y., & Zheng, Z. (2022). Temporal trends in the burden of non-communicable diseases in countries with the highest malaria burden, 1990–2019: Evaluating the double burden of non-communicable and communicable diseases in epidemiological transition. Globalization and Health, 18(1).https://doi.org/10.1186/s12992-022-00882-w
Ophori, E. A., Tula, M. Y., Azih, A. V., Okojie, R., & Ikpo, P. E. (2014). Current Trends of Immunization in Nigeria: Prospect and Challenges. Tropical Medicine and Health, 42(2), 67–75.https://doi.org/10.2149/tmh.2013-13
Policymakers in low- and middle-income countries (LMICs) are faced with numerous suggestions to boost economic growth and improve well-being. For instance, the United Nations’ Sustainable Development Goals outline 169 targets to achieve by 2030 (United Nations, 2015). These goals include providing free, fair, and high-quality primary and secondary education for all children, ensuring universal access to affordable and reliable energy services, decreasing global maternal mortality rates to below 70 deaths per 100,000 live births, and making significant reductions in marine pollution.
Even though all these objectives have the potential to enhance economic growth and quality of life, policymakers in LMICs are faced with difficult decisions when it comes to choosing which goals to prioritize due to budget limitations. Therefore, it is crucial to determine which investment priorities are most effective in promoting long-term economic growth and development.
Data constraints frequently hinder in-depth analysis of the macroeconomic impacts of precise, detailed policies. Although randomized controlled trials are valuable for identifying effective policies at a local level, extrapolating these findings to a broader scope is challenging due to the limited scalability of many programs (Deaton & Cartwright, 2018). Nevertheless, policymakers can still derive value from broad recommendations on the strategies most likely to support economic growth.
Countries such as Mexico, Indonesia, and Tanzania offer valuable case studies on the effectiveness of human development investments. This paper examines how these nations have approached human capital development and evaluates the extent to which these efforts have contributed to economic growth. By analyzing specific policies and programs, we will assess the role of education, health, and social welfare initiatives in fostering economic growth and offer recommendations for policymakers navigating similar challenges.
Human Development Policies: A Country Comparison
In economic theory, poverty traps refer to self-perpetuating conditions that keep populations impoverished. Two approaches have emerged to help countries escape these traps: investments in physical capital (such as infrastructure) and investments in human capital (including education, health, and social welfare) (Bloom et al., 2021). The ideal approach is an economic development strategy that combines a carefully prioritized number of infrastructure and human capital investments with best prospect of generating sustainable growth.
Mexico: Progresa and Seguro Popular
In Mexico, the Progresa program launched in 1997 targeted low-income families with conditional cash transfers tied to school attendance and health check-ups. The program’s design was groundbreaking in its emphasis on human capital development, and it succeeded in improving school enrollment and enhancing health outcomes (Behrman 2009). Exposure to Mexico’s Progresa program during childhood resulted in an increase of 1.4 years in average educational attainment. Girls were 30 percentage points more likely, while boys were 18 percentage points more likely, to obtain some secondary schooling (Parker & Vogl, 2018). More than two decades later, Progresa (now Prospera) continues to serve as a model for similar programs worldwide. However, some criticisms point to the program’s limited impact on breaking intergenerational poverty, particularly in rural areas where infrastructure is still lacking.
Seguro Popular, introduced in 2003, was another significant policy aimed at expanding healthcare access to uninsured populations. The program successfully reduced out-of-pocket healthcare expenditures and improved health outcomes, particularly among marginalized groups (Frenk, Gómez-Dantés, & Knaul 2009). However, Seguro Popular faced challenges in terms of sustainability and cost-effectiveness, leading to its eventual replacement in 2020 with Instituto De Salud Para El Bienestar (INSABI) (Unger‐Saldaña et al., 2023). The shift from Seguro Popular to INSABI reflects ongoing struggles with maintaining sustainable, large-scale healthcare programs. Political changes and fluctuations in government priorities have had a direct impact on the long-term sustainability of these programs.
Indonesia: PKH and JKN
Indonesia experienced a decrease in fertility rates from 1982 to 1987 due to investments in family planning programs and economic development. Gertler & Molyneaux (1994) findings showed that 75% of the decline in fertility was attributed to the increase in contraceptive use, which was mainly influenced by advancements in education and economic opportunities for women.
Indonesia has also pursued policies focused on human capital. The Program Keluarga Harapan (PKH), initiated in 2007, aimed to improve educational and health outcomes for low-income families through conditional cash transfers. Like Progresa in Mexico, PKH resulted in better educational achievements and reduced malnutrition (Banerjee et al. 2017). However, Indonesia faces unique challenges such as its vast geographical disparities and the difficulty of delivering services across the country (Moh Idil Ghufron & Ahmad Ali Bustomi, 2022).
Moreover, Jaminan Kesehatan Nasional (JKN), launched in 2014, has increased healthcare utilization and alleviated the financial burden of health expenses, but concerns remain about the program’s financial sustainability (Agustina et al. 2019). Rising healthcare costs and inadequate funding models have prompted debates about the long-term viability of JKN. Indonesia’s geographic challenges—spread across thousands of islands—compound this issue, leading to unequal healthcare access between urban and rural populations.
Tanzania: PSSN and CHF
Tanzania’s approach to human development also highlights the importance of well-targeted social welfare programs. The Productive Social Safety Net (PSSN), launched in 2012, provides conditional cash transfers to poor households. This program has increased school attendance and improved health outcomes among children and pregnant women (World Bank 2019). Yet, similar to Indonesia, Tanzania faces challenges in ensuring that remote and underserved communities can benefit from the program. Issues of access and service delivery are compounded by inadequate infrastructure and limited governmental capacity in some regions.
The Community Health Fund (CHF), introduced in 2001, aimed to provide affordable healthcare to the rural and informal sector populations (Wang et al., 2018). While the CHF has enhanced health security in some areas, its coverage remains incomplete, and many citizens still struggle to access quality healthcare (Borghi et al. 2013). The program’s reliance on voluntary contributions has also led to low enrollment rates, raising concerns about the fund’s ability to provide universal coverage.
Empirical Evidence: Quantifying the Impact of Human Development
The relationship between human development and economic growth is well-studied in economic literature. David Bloom and colleagues (2021) identified three key domains—education, health, and reproductive health—as having the most substantial impact on economic growth in LMICs. Their research shows that improvements in these areas are strongly correlated with increased economic growth.
By conducting cross-country and panel data regressions, they determined that enhancements in these areas have a positive influence on future economic growth. The following key findings are crucial for policymakers in LMIC settings to consider:
A decrease in the total fertility rate by one child corresponds to a 2-percentage point increase in annual GDP per capita growth in the short run and a 0.5 percentage point increase in the medium to long run (Bloom et al., 2021).
This dynamic is particularly relevant in countries like Indonesia, where high fertility rates have historically impeded economic growth. Policies promoting reproductive health and family planning have helped lower fertility rates, thus unlocking demographic dividends that contribute to economic growth.
A 10 percent rise in life expectancy at birth corresponds to a 1 percentage point increase in GDP per capita growth in the short term and a 0.4 percentage point increase over the long term (Bloom et al., 2021).
Increasing life expectancy has a direct effect on economic performance. In Mexico, Indonesia, and Tanzania, healthcare reforms such as Seguro Popular, JKN, and the CHF have improved population health and life expectancy, thereby contributing to higher productivity and economic stability.
A one-year increase in average years of schooling corresponds to a 0.7 percentage point increase in annual GDP per capita growth in the short term (Bloom et al., 2021).
The role of education in economic growth cannot be understated. In Mexico and Indonesia, conditional cash transfer programs like Progresa and PKH have contributed to higher school enrollment rates and reduced dropout rates, equipping future generations with the skills needed for productive employment. However, these programs also reveal limitations: while they improve access to education, they do not always address the underlying quality of education, which remains a concern, particularly in rural areas.
Economic Growth Through Human Development
Education plays a crucial role in driving long-term economic growth (Lutz et al., 2008). Individuals with higher levels of education tend to be more productive, earn higher incomes, and contribute more to overall economic output. However, in countries where fertility rates are high and families are large, there may be limited resources available to invest in each child’s education. This can lead to lower levels of education and lower earnings, which, in turn, can contribute to high fertility rates and large families in the next generation. This cycle can create a barrier to achieving sustained economic growth, as it hinders the transition to lower fertility rates and higher levels of education (Galor, 2011). This phenomenon, known as the fertility-induced poverty trap, is a significant challenge for low- and middle-income countries, preventing them from benefiting from the demographic dividend that comes with a shift in population age structure (Kotschy et al., 2020).
Moreover, unaffordable or low-quality education can hinder young people from developing the necessary job skills to improve their future earning potential. This cycle of limited education and low productivity can perpetuate poverty across generations, impede human capital accumulation, and restrict economic growth (Strulik et al., 2013).
In Mexico, Tanzania, and Indonesia, investments in education have led to better educational outcomes and higher productivity. Conditional cash transfer programs such as Progresa and PKH were instrumental in raising school enrollment rates and reducing dropout rates, ensuring that future generations possess the skills necessary to contribute to the workforce.
The Role of Health in Economic Development
Poor health conditions and high rates of infectious diseases can trap populations in poverty, as unhealthy individuals are less likely to invest in education or productivity-enhancing activities. In Tanzania, for instance, policies focused on improving maternal and child health have played a critical role in improving human capital. Tanzania’s Community Health Fund (CHF), which aims to provide affordable healthcare to rural and low-income populations, has led to significant improvements in population health, further contributing to the economic stability of the population (Borghi et al., 2013).
Individuals with poor health may have a lower life expectancy, making it less likely for them to benefit from investments in education (Cervellati & Sunde, 2013). As a result, private investments in education may not be seen as worthwhile, and public investments in education may not be fully utilized due to low demand. Poor health and its subsequent lack of access to education can limit a country’s potential for economic growth (Bloom et al., 2020).
Moreover, a lack of family planning in Indonesia have been associated with decreased economic stability. Kim et al. (2009) showed that the arrival of a newborn child in an Indonesian household led to a 20% decrease in household consumption per person over four years. As such, in countries like Indonesia, policies aimed at promoting reproductive health have contributed to reductions in total fertility rates, which in turn has contributed to economic growth.
Critical Analysis and Challenges
Across these countries, similar limitations arise. Progresa and PKH succeed in improving access to education and health services but struggle with the quality of services in rural areas. Yet, limited infrastructure, such as schools and healthcare centers, hinders the effectiveness of these programs.
In Mexico, INSABI, which replaced Seguro Popular (Unger‐Saldaña et al., 2023), has yet to prove whether it can maintain a sustainable healthcare system that reaches all populations. Meanwhile, Indonesia’s JKN faces increasing financial pressures, especially considering the informal sector unwillingness to pay for it (Muttaqien et al., 2021).
In all three countries, a lack of investment in infrastructure—whether physical or digital—limits the success of human capital programs. For instance, rural communities often lack electricity, internet access, and transportation, which are essential for both education and healthcare services.
Exploring Other Dimensions of Human Development
Beyond education, health, and reproductive health, several other dimensions significantly influence human development outcomes in LMICs:
Nutrition: Malnutrition continues to be a critical issue in LMICs, where large rural populations face food insecurity. Poor nutrition, especially in early childhood, can result in long-term health issues and impede cognitive development, directly affecting educational outcomes and economic productivity (Ekholuenetale et al., 2020).
Gender Equality: Women’s access to education and healthcare is essential to driving down fertility rates and increasing economic participation. Programs that focus on maternal health and girls’ education in LMICs have shown success in improving gender equity, but challenges remain, particularly in rural areas (United Nations, 2020).
Technology Access: Access to technology is becoming an increasingly important factor in both education and healthcare. The digital divide between urban and rural populations in LMICs can limit the potential benefits of human development programs. For example, telemedicine and online education initiatives can help bridge the gap (Dillip et al., 2024).
Additionally, collaboration with international institutions has been used by Tanzania, Indonesia, and Mexico for a push to development in some contexts. Mexico’s entry into the Organisation for Economic Co-operation and Development (OECD) in 1994 led to economic and social reforms aligning with OECD standards, resulting in gradual improvements in human development indicators such as literacy rates and life expectancy (OECD, 1997). Indonesia’s ASEAN membership since 1967 facilitated regional cooperation, enhancing education, healthcare, and infrastructure, and driving human development (Lorraine Pe Symaco & Meng Yew Tee, 2019) Tanzania’s membership in the East African Community (EAC) since 2000 has promoted economic integration and social development (Drummond, 2015).
Conclusion
Investments in human capital—particularly in education, health, and reproductive health—are crucial for driving sustained economic growth in LMICs. The experiences of Mexico, Indonesia, and Tanzania demonstrate the potential of well-targeted human development policies to improve economic outcomes. However, these efforts must be complemented by critical investments in infrastructure, based on a country’s context, and must address national inequalities to achieve their full potential. Policymakers in LMICs should prioritize long-term strategies that integrate human development with infrastructure improvements, ensuring that gains in education and health translate into broad-based economic growth.
References
Agustina, R., Dartanto, T., Sitompul, R., Susiloretni, K. A., Suparmi, Achadi, E. L., Taher, A., Wirawan, F., Sungkar, S., Sudarmono, P., Shankar, A. H., Thabrany, H., Agustina, R., Dartanto, T., Sitompul, R., Susiloretni, K. A., Suparmi, Achadi, E. L., Taher, A., & Wirawan, F. (2019). Universal health coverage in Indonesia: concept, progress, and challenges. The Lancet, 393(10166), 75–102. https://doi.org/10.1016/s0140-6736(18)31647-7
Banerjee, A. V., Hanna, R., Kreindler, G. E., & Olken, B. A. (2017). Debunking the Stereotype of the Lazy Welfare Recipient: Evidence from Cash Transfer Programs. The World Bank Research Observer, 32(2), 155–184. https://doi.org/10.1093/wbro/lkx002
Behrman, Jere R, et al. (2009). Schooling Impacts of Conditional Cash Transfers on Young Children: Evidence from Mexico. Economic Development and Cultural Change, 57(3), 439–477. www.ncbi.nlm.nih.gov/pmc/articles/PMC2832207/
Bloom, D. E., Kuhn, M., & Prettner, K. (2020). The contribution of female health to economic development. The Economic Journal, 130(630), 1650–1677.
Bloom, D. E., Khoury, A., Kufenko, V., & Prettner, K. (2021). Spurring economic growth through human development: research results and guidance for policymakers. Population and Development Review (2021).
Borghi, J., Maluka, S., Kuwawenaruwa, A., Makawia, S., Tantau, J., Mtei, G., Ally, M., & Macha, J. (2013). Promoting universal financial protection: a case study of new management of community health insurance in Tanzania. Health Research Policy and Systems, 11(1). https://doi.org/10.1186/1478-4505-11-21
Cervellati, M., & Sunde, U. (2013). Life expectancy, schooling, and lifetime labor supply: Theory and evidence revisited. Econometrica, 81(5), 2055–2086.
Dillip, A., Kahamba, G., Sambaiga, R., Shekalaghe, E., Ntuli Kapologwe, Kitali, E., James Tumaini Kengia, Tumaini Haonga, Nzilibili, S., Tanda, M., Haroun, Y., Hofmann, R., Litner, R., Riccardo Lampariello, Suleiman Kimatta, Sosthenes Ketende, James, J., Khadija Fumbwe, Mahmoud, F., & Lugumamu, O. (2024). Using digital technology as a platform to strengthen the continuum of care at community level for maternal, child and adolescent health in Tanzania: introducing the Afya-Tek program. BMC Health Services Research, 24(1). https://doi.org/10.1186/s12913-024-11302-7
Ekholuenetale, M., Barrow, A., Ekholuenetale, C. E., & Tudeme, G. (2020). Impact of stunting on early childhood cognitive development in Benin: evidence from Demographic and Health Survey. Egyptian Pediatric Association Gazette, 68(1). https://doi.org/10.1186/s43054-020-00043-x
United Nations. (2015). The 17 Sustainable Development Goals. United Nations.
United Nations. (2020). World Fertility and Family Planning 2020. UN Report.
World Bank Group. (2019, September 16). Five Million Tanzanians to Benefit from Improved Safety Nets. World Bank.
Appendix
Graph 1: Tanzania’s Correlation Matrix
Graph 2: Mexico’s Correlation Matrix
Graph 3: Indonesia’s Correlation Matrix
Benita Kayembe,
Senior Program and Research Coordinator
Despite seemingly insurmountable odds, on November 15, 2022, the Parliament of Sierra Leone passed the Gender Equality and Women’s Empowerment Act (GEWE). Passage of this historic legislation was the culmination of two years of indefatigable effort and astute political strategy by the Minister of Gender and Children’s Affairs, Manty Tarawalli.
Background
Despite seemingly insurmountable odds, on November 15, 2022, the Parliament of Sierra Leone passed the Gender Equality and Women’s Empowerment Act (GEWE). Passage of this historic legislation was the culmination of two years of indefatigable effort and astute political strategy by the Minister of Gender and Children’s Affairs, Manty Tarawalli.
Even though women in Sierra Leone are 52% of the population, they face many discriminatory practices related to customary law in areas such as marriage, divorce, inheritance, and family relations, highlighting unequal rights, roles, and socio-economic outcomes.2 When President Julius Maada Bio was elected in 2018, only 11% of parliamentary seats were held by women. Moreover, Sierra Leonean women were disproportionately less likely to access post-secondary education and to own assets such as radios, mobile phones, and bank accounts, and the country was ranked 114th out of 149 countries on the Global Gender Gap Index.3
The historical context of Sierra Leone, tainted by colonialism and further exacerbated by the brutal civil war of 1991-20022, contributed to the entrenched gender inequalities in the country. Emerging from the ashes of the 11-year civil war that wreaked havoc on every facet of the nation’s well-being, Sierra Leone confronted the colossal task of rebuilding its social, economic, and physical infrastructure.
Despite various non-government initiatives and efforts by the few women in Parliament, women in Sierra Leone still grappled with deeply entrenched historical challenges, including limited access to education and economic opportunities, as well as gender-based violence.4,5 To tackle issues adversely affecting women and children, President Bio, in 2019, established the Ministry of Gender and Children’s Affairs. At its head, he nominated Manty Tarawalli, whose well known commitment to sustainable and gender-equitable development became priorities.
As head of the Ministry of Gender and Children’s Affairs, Manty Tarawalli’s efforts to help rebuild gender equity in the nation were multi-dimensional, encompassing the collaboration of various governmental sectors and civil society. This case study examines the trajectory of her leadership, beginning with the inception and extending to the coordination of national and regional entities cumulating in the successful enactment of the Gender Equality and Women’s Empowerment (GEWE) Act.
The Minister’s Goal
Upon assuming office in 2020, Manty set her ministry’s goal to improve gender equality in Sierra Leone by increasing women’s representation in the public and private sectors to 30%. She believed that by doing so, women would be empowered to live their rights and socio-economically support themselves, their families, and the country.
Manty’s goal to increase women’s representation in both the public and private sectors to 30% was rooted in President Bio’s 2018 election manifesto. During the election campaign this manifesto garnered widespread support, signifying a desire for a positive transformation in the status of women within the country.
A Bill to be Introduced: A Controversial Endeavor
Prior to Manty’s appointment as Minister of Gender and Children’s Affairs, various initiatives focused on women’s empowerment were already underway in Sierra Leone. Nevertheless, the perception of women’s empowerment initiatives was unfavorable to many due to misconceptions held by both men and women that gender equality efforts aimed for a strict 50/50 arrangement of power, potentially resulting in women assuming total control.
Historically, Sierra Leone had a prevailing male dominance in all key positions and every facet of its society. When President Bio was elected, the percentage of women Members of Parliament stood at a mere 11%. Aspiring to promote women’s participation in the public and private sectors to 30%, especially in Parliament, was complicated by the limited overall seats available. This initiative meant reshaping the composition of Parliament, as well as other sectors. Men who predominantly held executive, governmental, and leadership positions were unwilling to relinquish their place at the table in order to reserve 30% for women, making the prospect of a GEWE Act controversial.
A Leader’s Support as the First Step: The President of the Republic
Because of the far-reaching implications of the initiative under discussion, the Minister recognized that her goal could only be realized through legislation. The Minister also recognized that this goal required full support from the President of the Republic. She said:
“I needed to hear ‘I support your goal’ from the President. That is all I needed. I knew the road would not be easy, but I knew I could make it with support from the first man in the country.”
Seeking the President’s support, Manty met with him to deliberate on her objective, underscoring its alignment with the President’s manifesto. Unequivocally, the President endorsed the Minister’s goal and strategy.
From the President’s perspective: “Structural and cultural limitations had hindered women’s involvement in various areas in Sierra Leone, including education and development.” His perspectives on the issue were shaped by the formative role in his life of his mother and sister. Therefore, during his presidency, he was committed to dismantling ingrained societal biases and demonstrating unequivocally that women possess equal abilities and may even surpass men in certain aspects. In President Bio’s words:
“I firmly believe that involving women in decision-making brings diverse perspectives. Their participation leads to well-rounded decisions, which is crucial at the national level. Now, I trusted the Minister to lead us toward that.”
“After receiving the ‘I support this goal’ from the President,” Minister Manty said, “my ministry decided to put a GEWE Bill together.”
Strategic Key Collaborators
Alongside the backing of the President, Manty strategically identified and enlisted vital collaborators to champion the enactment of the GEWE. She extended her outreach to engage prominent female politicians, lawmakers, gender activists, and the UN Women, among others. In Sierra Leone’s context, these key collaborators wielded significant influence that extended across the country. They were pivotal in providing counsel, outreach, and financial support for the logistics involved in lobbying and motivating public support for the proposed GEWE Bill.
Steps to Making a Law in Sierra Leone
In Sierra Leone, when a Bill originates from the executive branch of the government, it is referred to as a government Bill. This Bill must then be presented in Parliament by the Minister who holds jurisdiction over the subject matter. The following are the steps of how a Bill becomes a Law in Sierra Leone:
Table 1: How a Bill Becomes a Law in Sierra Leone6
Initiation of a Bill to be introduced from the executive arm of government
Encapsulate the policy of the government
Introduce the policy to the Cabinet for deliberation
The cabinet approves the government Bill after deliberation, and it goes to Parliament for the legislative stages
Stage 1: Notice regarding the Bill being introduced
The Bill is published in at least two issues of the gazette 9 days before first reading
Minister or Members of Parliament (MPs) sends a memo explaining the objects and reasons for the Bill
Parliament holds pre-legislative consultation with the Minister or MP in charge of the Bill
Stage 2: Introduction and first reading
The Minister or MP moves the motion for the first reading
The Clerk reads short title of the Bill to Parliament
Stage 3: Second reading
Clerk reads long title of the Bill to Parliament
MPs debate the merits and principles of Bill
Stage 4: Committee stage
Detailed discussion of Bill
Sittings may include public hearings
Relevant amendments are made
Bill is reported to the Committee of the Whole House
Stage 5: Third reading
Parliament amends errors and review Bill
Bill is read for the third time, including any amendments
Bill passed to law in parliament
Stage 6: President’s assent
The president of Sierra Leone signs the Bill
Stage 7: Publication in gazette
Bill becomes law on the day it is published in the government Gazette
A Government Bill Policy: No Backing from Your Own Political Party
“So, how do we meticulously construct the Bill?” Manty said, “The process involved a collaborative effort, bringing various partners together.” Manty diligently engaged legal practitioners and lawyers. Through comprehensive meetings and thorough studies, they endeavored to gain insights from countries that had already embarked on similar initiatives, mainly learning from their strategies for garnering significant female participation in their Parliament. According to Neneh Lebbie, the President of the Parliamentary Female Caucus:
“This investigative approach proved highly valuable, leading to uncovering methods that were instrumental in increasing the involvement of women in politics.”
These learnings helped further inform discussions about the proposed Bill. However, when the draft Bill was presented to the Cabinet for initial deliberation, Cabinet Ministers, for the first time, voiced their concerns about the transformative implications of the proposed legislation. Manty said:
“The preceding work happened behind the scenes within the ministry, while here is where I was showing my head. Now, having assumed my role in the Cabinet as a new Minister, I presented the proposal with enthusiasm. However, to my dismay, it faced a severe setback. It was met with opposition, leading to its thorough dissection and eventual rejection.”
In a disheartening testimony to resistance to the legislation, the Cabinet deemed reserving a 30% quota for women unattainable. At this first deliberation, the resounding message from Cabinet Ministers was that a transformative approach for women should not merely involve slotting them into existing positions; this would mean removing some men from their seats. Instead, the focus should be cultivating opportunities that defy traditional gender roles. Manty said:
“No man was willing to leave and give their seat to a woman. The Cabinet chopped this Bill to death. This was my own Party, and they chopped it out. They said absolutely no to 30%. I was down, and I took two weeks to recover. Then I got up again. And then, we started with a different approach. Now, I went to speak to each Cabinet Minister independently.”
Communicating the Vision to Cabinet Members: A One-on-One Approach
Following initial rejection by the Cabinet, Manty recognized the necessity for a fresh approach to securing Ministers’ support for the Bill. With this objective in mind, she embarked on individualized discussions, engaging in one-on-one conversations with each Cabinet Minister. She meticulously presented her case to every Minister, articulating compelling arguments tailored to their perspectives and concerns. In Manty’s words, she told every Cabinet member that:
“As Cabinet members, our goal is clear—we aspire to elevate our nation to a middle-income country. In this pursuit, the integration of women in leadership positions is indispensable. It is imperative to recognize and harness women’s diverse skill sets. Women have unique perspectives and contributions that are distinct from traditional male leadership. This assertion about women in leadership positions is substantiated by data that indicate that such an approach is beneficial and integral to our country’s growth trajectory. Nations that have successfully transitioned to middle-income status have actively integrated women into leadership roles.”
Subsequently, the proposed legislation underwent a second presentation in the Cabinet. Now, there was a palpable sense of optimism regarding the potential for the policy to earn the Cabinet’s endorsement. As the second deliberations commenced, the first Minister to speak expressed his support for the proposed legislation and set the stage for a productive discourse. Manty elaborated:
“An eminent figure, formerly Minister of Information and now serving as the Minister of Labor, was first to respond and comment on the Bill. I recall engaging in a thoughtful exchange when we convened in his office. Now, he was in full support of the Bill. There, he told Cabinet members that Minister Manty presented comprehensive information and data that unveiled a compelling growth narrative if we were to bring more women into leadership positions. Witnessing what she presented, I experienced a profound shift in perspective. It was an introspective moment, and while I recognize that the decision might personally impact me, the overarching impact of a GEWE Act would propel our nation forward. I support this Bill.”
This was a pivotal moment, and in response to this powerful first statement, Manty said: “His Excellency (the President) smiled.”
Consequently, more Ministers voiced support for the proposed legislation, and a government Bill came out of the Cabinet. To tell the population what had happened on that day, Minister Manty explains:
“It was phenomenal. I do not usually go to social media, but I went there and informed the population of what had happened that day. A wave of endorsement of the Bill surged across social media platforms. The resonance was palpable as individuals from all walks of life enthusiastically rallied around this triumphant moment.”
From the Cabinet to the Parliament: Parliamentarians Decide
The next step involved presenting the government Bill to Parliamentarians. In Sierra Leone, the Parliament operates independently from other decision-making bodies. With the submission complete, the Bill’s fate lay in the hands of the Parliament. Considering that the Minister’s political Party did not hold the majority in the Assembly, support from some opposition members would be needed. At the outset, opponents in Parliament were categorized as follows:
A surprising fraction of women, although a minority, embarked on opposing the initiative. Their stance pivoted on the notion that making the path easier for other women would undermine the essence of strength and perseverance that define female leadership. Their perspective advocated that if a woman aspires to lead, she should earnestly strive and demonstrate her merit. No one should give her a seat at the table.
With a pointed reminder of their historical commitment to this cause, some women in Parliament were opposed to Manty’s leadership, especially as a new Minister. They asserted that their contributions over the years rendered them the rightful torchbearers of this movement.
Many men in Parliament and members of opposing political Parties were unwilling to give up their seats for women nor let their political opponents win.
Others said they could not oppose their esteemed political elders, even when personal convictions diverged.
Using Human Rights Arguments: Partners Needed Everywhere
At the beginning stages of the legislative process in Parliament, Minister Manty and her key collaborators advocated for the Bill by highlighting human rights arguments. These arguments underscored the fundamental principle that every woman has the inherent right to determine her identity and aspirations and that gender equality and women’s empowerment would positively impact Sierra Leone society.
However, using human rights arguments, the Bill encountered resistance. Counterarguments against the human rights notion were rooted in skepticism, suggesting Minister Manty was injecting personal viewpoints into her political objectives. A factor in these negative perspectives was subjective perceptions such as the Minister’s foreign education and accent, portraying them as evidence of the foreign influence she was bringing to her ministerial ambitions. They posited that she was trying to impose Western ideals onto Sierra Leone’s cultural fabric, implying a potential disruption to their traditional norms. For many parliamentarians, it was a no for the GEWE Bill.
At this stage, continuing to use human rights arguments meant failure in Parliament. Consequently, Manty began considering the multifaceted dynamics at play and the differing viewpoints in the private and public sectors regarding women’s empowerment. Switching tactics, the Minister began advocating for her goals using economic instead of human rights arguments.
Using Economic Arguments: Partners Needed Everywhere
Manty and her key collaborators leveraged economic arguments to garner more support, highlighting that the GEWE, if enacted, would elevate Sierra Leone into the ranks of a middle-income country. They argued that this transformative Bill would echo within every household in Sierra Leone by increasing income, potentially improving every aspect of life in the country. Using economic arguments, the conversation began to change, and more were willing to engage in favorable conversations about the Bill.
According to the Vice President, Mohamed Juldeh Jalloh, the economic discourse struck a chord with many. They envisioned households flourishing as women contributed more substantially to their communities’ development. The economic message was a compelling call to action that appealed to everyone across genders. In the Vice President’s words:
“Empowerment is not representation; it is economic uplifting. People understood they could reduce their dependence and vulnerability if more women were empowered.”
From Vice President Mohamed’s standpoint, the economic discourse developed a movement for women and girls in the country, mainly supported by President Bio’s Manifesto and commitment to women’s equality. Vice President Mohamed said:
“The President wanted to bring gender in all aspects of the country, and that is what we began to work on. We were set to create conditions for women to suffer less.”
While parliamentarians were still deliberating the Bill, President Bio’s administration increased the budget for girls’ education to 22%, STEM education became free for every girl in the country, energy access was brought to many women’s markets, an ambulance to primarily serve pregnant women was made available in every district, and budget allocation to decrease maternal mortality in the country increased from 6% to 11%. From President Bios perspective, working on resolving issues faced by women, as communicated in his manifesto, even without the GEWE Act, was a way to show the populace what more could be possible if the GEWE was enacted. In Vice President Mohamed’s words:
“We created the noise. Politics must be noise. Strategically understand public opinion and reflect the needs of the people.”
From the opposition standpoint, Emerson Lamina, an opposition leader in the Parliament of Sierra Leone, elaborated that:
“This approach underscored the need for collective action to support national goals. Two key values that emerged from the President’s initiatives were empathy and equality. His efforts included reducing school fees for girls, addressing sexual violence, and declaring a state of emergency to combat rape. These actions resonated with my 23-year journey advocating for women’s rights.”
Emerson further explained that to support the President’s vision, he transitioned from an opposition position to a supporting one. According to him, dialogue, consensus-building, negotiation, and partnership were crucial strategies employed by Minister Manty and proponents of the Bill. They recognized the need for representation from various Parties and beliefs, facilitating a more inclusive approach to supporting women.
Parliamentarians Still Not Supporting the GEWE Bill: What Next?
Despite positive momentum, the Bill hit another roadblock when parliamentarians raised concerns that the GEWE Bill was discriminatory. They argued, mandating a 30% quota for women raised concerns about the Bill’s constitutionality because the legal framework in Sierra Leone strongly opposes any form of discriminatory legislation. Consequently, according to them, the call for men to abstain from contesting all available seats by reserving 30% to women, especially within the Parliament, was discrimination.
However, according to the Parliament’s Speaker Abass Bundu:
“Not every aspect of the Bill was considered discriminatory. The argument arose whether preferential treatment should be given to either sex. This issue prompted discussion on the practicality and fairness of such provisions, and we realized that specific conditions were needed to address concerns about fairness.”
In this context, the insights of the Parliament’s Speaker emerged as pivotal. His counsel to the proponents of the Bill consisted of the following key points:
Conduct a comprehensive analysis of Sierra Leone’s laws to identify potential ambiguities that could be leveraged.
Engage directly with the people who elect the parliamentarians, bypassing the need for solely parliamentary deliberation.
Undertake a thorough rewording and revision of the Bill to ensure alignment with the principles of fairness and equality.
In response to the Speaker’s advice, the Bill underwent further revisions. The process also involved more comprehensive public consultation to gather perspectives and address concerns. This process intensified over 13 months, during which the Bill was being revised and deliberated in Parliament.
Comprehensive Analysis of Sierra Leone’s Laws: Ambiguities to Leverage
While conducting an extensive review of Sierra Leone Constitution, proponents of the Bill discovered a pivotal clause within the Constitution of Sierra Leone (Amendment) Act of 2001. This clause made provision for a District Block System, a form of Proportional Representation Elections System, which served as the foundation for several key provisions outlined as follows:
(1) A candidate shall be nominated in writing by 3 voters of the electoral area for which he intends to contest an election and shall not be in more than one electoral area
(2) For every 3 candidates nominated under subsection (1), one of them shall be female
(7) On the delivery of the nomination paper together with prescribed nomination fee, the returning Officer for the electoral area shall for with acknowledge receipt of the nomination paper and nomination fee:
Provided that the returning officer shall reject the Nomination of Candidate made in contraction of subsection (2)
Consequently, the Bill shifted from asking for a strict 30% quota for females to proportional representation. The change in terminology effectively addressed the concerns about discrimination that some parliamentarians had. The revised Bill stated that for every two male candidates nominated in any given district, the third nominee should be female. Similarly, in any public or private sector, the third appointee should be female for every two males appointed.
This shift marked a departure from an inflexible quota system to a more proportional representation approach. Nonetheless, while employing the proportional approach, the Bill, if enacted, would still ensure at least 30% female representation across all sectors.
Simultaneous with the legislative process, comprehensive public consultation was underway to incorporate diverse viewpoints, and address concerns regarding the Bill.
Consulting with the Population: A Bill by Them and for Them
While advocating for the enactment of the GEWE Bill, Minister Manty and her key collaborators used various platforms, including print, social media, radio, and television, to disseminate positive messages regarding the proposed Bill. Their approach involved sharing educative content through impactful infographics via social media, as well as information snippets through the radio. Neneh Lebbie, the President of the Parliamentary Female Caucus, said:
“Radio, in particular, emerged as an invaluable tool due to its widespread popularity among villagers, who attentively tuned in and frequently discussed broadcast contents with peers.”
In this way, proponents of the Bill initiated a national dialogue that rippled through society. Manty went to every district in Sierra Leone to meet with the population. She also went to remote villages and communities and visited schools throughout the country to comprehensively address people’s issues and improve the proposed Bill based on their input. Where needed, she relied on village leaders to convey her message to their peers.
Everywhere Manty went, she first introduced herself as a wife to address issues regarding her foreign influence and reassure those arguing that women would no longer want to assume their roles as wives and mothers if empowered. She told everyone:
“A man is a household’s sole breadwinner, responsible for feeding ten mouths. However, if his wife starts working in income-generating activities, their household will have more money to subsist.”
To appease husbands’ fears, she told their wives:
“Do not misappropriate my advocacy to justify disrespecting your partner.”
Manty underscored the Bill’s importance to households and Sierra Leone’s economic growth everywhere she went. This Bill, she explained: “meant a thriving home and a thriving nation.”
Cross-Collaboration
According to UN Women Country Director, Setcheme Mongbo, collaboration between UN Women and Manty’s ministry aimed at mainstreaming the GEWE Bill within ministries was crucial. The role of UN Women extended beyond public visibility and included crucial behind-the-scenes interactions such as connecting Minister Manty with opportunities for grants for logistical support or meeting with stakeholders who had questions about indicators around gender equality or women’s status in society. In Setcheme Mongbo, the UN Women Country Director, words:
“This required patience, negotiation, and dialogue to facilitate collective understanding and ensure all stakeholders aligned with the goal.”
Another collaborator, Nicky Spencer-Coker, a radio host, practicing barrister, and solicitor of the High Court of Sierra Leone, explained that this Bill presented a window for many gender equality advocates to advance the position of women and girls in Sierra Leone. In her words:
“This Bill served as a blueprint for advancing girls’ and women’s development and promoting a feminist perspective in all aspects of life. Women organizations, women rights activists, and feminists had worked tirelessly for these advancements. However, it required significant political will and leadership to unify these efforts into a coherent vision for the country.”
With Minister Manty leading the movement, Nicky and other collaborators such as Neneh Lebbie, the President of the Parliamentary Female Caucus, joined in by providing legal counsel and other logistical and technical support throughout the legislative process.
Gradually, collaboration between the Ministry of Gender and Children’s Affairs, other Ministries, prominent female politicians, lawmakers, gender activists, the UN Women, and others brought the country together to improve Sierra Leonean women’s lives. Manty and her collaborators met with the opposition when needed, answered questions from the population, and worked to bridge communication gaps between opponents and proponents of the Bill, garnering more support for the enactment of the GEWE Bill.
The Gender Equality and Women’s Empowerment (GEWE) Act of 2022
By engaging every corner of the country, navigating complex negotiations, and cultivating alliances, the GEWE Bill, step by step, garnered greater support among citizens and parliamentarians. In Manty’s words: “It was an arduous path that embodied challenges and resilience.”
Despite initial resistance, the GEWE Bill was ultimately enacted in parliament with 100% support from parliamentarians. After President Bio had signed, it was published in the Government Gazette on December 30, 2022 and finally became law.
Inter-ministerial collaboration can take a number of forms, varying greatly in commitment and scale. A ministry’s commitment to collaboration can range from informal to formal and the scale of collaboration can range from bilateral to whole-of-government.
Commitment
Informal
Intermediate
Formal
Unofficially Recognized, Non-Binding
Officially Recognized, Non-Binding
Officially Recognized, Legally Binding
Scale
Bilateral
Sectoral
Whole-of-Government
Cooperation of 2 ministries
Cooperation of 3+ ministries (with related interests)
Cooperation of many ministries to implement a coordinated national strategy aimed at achieving a major national goal
Why Collaborate?
There are significant advantages to working across ministries in various situations, but inter-ministerial collaboration defies the traditional silo organization of government. Changing the way government usually works is not easy and should be deliberately planned and diligently managed if it is to be effective.
Benefits
Optimize use of public resources
Combine and amplify related skills and capacities
Welcome a wider inclusion of perspectives into the policymaking process and increase the degree to which policies reflect the will of the public by involving previously unheard perspectives
Increase clarity surrounding roles, responsibilities, goals, and mission
Increase the satisfaction of constituents and enthusiasm of staff
Barriers
Challenging to ensure shared ownership for inter-ministerial collaboration
Overlapping jurisdiction between ministries
Unwillingness of some ministers and other government officials to relinquish and share power over decision-making and agenda-setting processes
Lack of clearly operationalized collaboration plans
When to Collaborate:
Ministers should be routinely on the lookout for opportunities to advance their specific policy goals or national priorities through closer collaboration with other ministries or government agencies. Such opportunities may be relatively modest, focusing on one particular part of a bigger undertaking, or it could be jointly implementing a major complex program. In evaluating opportunities for inter-ministerial collaboration, ministers should consider the following key factors:
Considerations
Length of goals to be achieved: Opportunity to formalize medium to long term engagement between ministries towards a common goal
Level of information sharing required: Opportunity to integrate, share, and better validate data from different sources
Level of existing collaboration: Opportunity to build on existing institutional relationships
Required budgetary resources: Opportunity to consolidate resources to be used more efficiently
Required skills and capacity: Opportunity for peer learning and knowledge sharing across ministries
Required political capital: Opportunity to break through the status quo and accomplish meaningful institutional and sectoral change but sufficient risk tolerance needed
How to Collaborate:
The sustainability and success of a collaborative partnership fundamentally depends on the amount of time and effort invested in setting up the partnership, instituting the most practical organizational structure to oversee and implement the initiative, and consistent ministerial leadership. Clear lines of responsibility and accountability are essential. The following are key factors for the success of inter-ministerial collaboration:
Enabling Factors
Existence of strong and sustained ministerial initiative to drive process
Detailed, inclusive planning before implementation
Clear roles, routines, and lines of accountability for all parties
Relentless consultation to ensure inclusive input and generate cultural buy-in
Downstream collaborative routines and structures at regional levels when required
Designated budgetary resources pooled and allocated to a singular plan
1. WHY COLLABORATE? EVIDENCE FOR INTER-MINISTERIAL COLLABORATION
“…collaboration is capable of addressing complex social problems more effectively than ever before, achieving more and better outputs and outcomes for individuals and their families, empowering communities to be more self-reliant, and creating a more inclusive and coordinated public sector.”
-Debiprosad Majumdar, Social Policy Journal of New Zealand (2006)
As collaborative efforts in countries of varying cultural, historical, and economic backgrounds have gained more recognition, common learnings have emerged. This section sets out the evidence about inter-ministerial collaboration regarding varied approaches, benefits, and barriers for consideration by government leaders regardless of their country’s governance system or size of government.
Approaches to Inter-Ministerial Collaboration
Inter-ministerial collaboration can take a number of forms, varying in commitment and scale (Dill & Kopsick, 2017; Colgan, Kennedy, & Doherty, 2014). A ministry’s commitment to collaboration can range from the informal to the formal as outlined in Table 1. The scale of inter-ministerial collaboration ranges from bilateral to whole-of-government as outlined in Table 2.
Table 1. Levels of Commitment in Inter-Ministerial Collaboration
Commitment
Description
Informal
Unofficially Recognized, Non-Binding E.g. Unscheduled, periodic sharing of information
Intermediate
Officially Recognized, Non-Binding E.g. Memorandum of understanding
Formal
Officially Recognized, Legally Binding E.g. Collaboration enshrined in law
Adapted from Dill and Kopsick, 2017
Table 2. Levels of Scale in Inter-Ministerial Collaboration
Scale
Description
Bilateral
Cooperation of two ministries
Sectoral
Cooperation of three or more ministries (typically those with related interests)
Whole-of-Government
Cooperation of many ministries to implement a coordinated national strategy aimed at achieving a major national goal
There is no single way to collaborate effectively. Ministers can select the form of collaboration – with regards to level of commitment and scale – that is most appropriately suited to their goal. As an example, Table 3 outlines multiple forms of inter-ministerial collaboration across the spectrums of scale and commitment that could be implemented by a government looking to improve its youth health outcomes.
Table 3. Example Demonstrating Various Forms of Inter-Ministerial Collaboration to Improve Youth Health Outcomes
Scale
Informal
Intermediate
Formal
Whole-of-Government
In their inaugural address, the Prime Minister asks ministry leaders to prioritize sharing of data related to youth health across ministries
The government submits a proposal soliciting international funding that will be used to create an integrated, cross-government data platform to better monitor youth health outcomes and other relevant data across all sectors
The Prime Minister declares improvement of youth health to be a national priority in the country’s national economic development plan and ties significant national-level funding to one inter-ministerial plan to improve youth health indicators
Sectoral
The Ministries of Education, Health, and Housing grant respective Deputy Ministers access to data focused on youth health
The Ministries of Education, Health, and Transportation draft and sign a non-binding agreement to share responsibility in ensuring youth have physical access to affordable healthcare
The Ministries of Education, Health, Sport, and Agriculture are required by legislation to contribute representatives to a taskforce aimed at reducing rates of childhood obesity
Bilateral
The Ministry of Education agrees to exchange student health data with the Ministry of Health on a quarterly basis
The Ministry of Education signs a MOU with the Ministry of Health to create a taskforce and conduct research on the integration of healthcare services into schools
Parliament passes a law mandating collaboration between the Ministry of Health and the Ministry of Education to improve youth health, requiring monthly reports detailing the outcomes
Benefits of Inter-Ministerial Collaboration
When implemented with sufficient ministerial commitment and a clearly operationalized collaboration plan, the benefits of inter-ministerial collaboration can significantly bolster existing ministerial efforts and create long-lasting institutional change. Effective collaboration between ministries can achieve numerous benefits as outlined below:
Optimize use of public resources: Given the interrelated nature of most human development challenges, a key benefit of collaboration is its ability to use budgets for intersecting programs that overlap, allowing for more efficient use of public funding. Furthermore, improving returns on investment can motivate greater investment for future programs, from both domestic and international sources (Majumdar, 2006).
Combine and amplify related skills and capacities: Collaboration across ministries requires ministry officials to plan and implement together, prompting learning about each other’s sectoral considerations and developing intersectoral capabilities that support more effective and comprehensive programs (Wanna, 2008).
Welcome a wider inclusion of perspectives into the policymaking process, thereby increasing the degree to which policies reflect the will of the public: Inter-ministerial collaboration forces decision makers to hear varying perspectives and weigh costs and benefits beyond their sector – this is a decision-making process that better reflects human development and societal interactions (Wanna, 2008).
Increase clarity surrounding roles, responsibilities, goals, and mission: Tasks are more likely to be accomplished when the path to completion is reached together, when lines of accountability are rigid, and when communication plans are clear among all collaborating parties (Majumdar, 2006).
Increase the satisfaction of constituents and enthusiasm of staff: Ministry staff feel pride in delivering services in a more efficient way while constituents notice and appreciate integrated public services and effective public spending (Roberts & O’Connor, 2007).
Barriers to Inter-Ministerial Collaboration
Inter-ministerial collaboration has the ability to expand the quality and reach of government services. To achieve this potential, however, ministers must be prepared to identify and address complex challenges.
Even the most well-intentioned collaborative effort can fall victim to these common barriers:
Ensuring shared ownership for inter-ministerial collaboration can be challenging: While effective inter-ministerial collaboration requires clear leadership and lines of accountability, there is also a need for shared ownership to ensure that collaborative efforts are prioritized and ministerial obligations are met. Sharing credit among ministries is critical to ensure shared reward but also shared responsibility for collaborative implementation.
Presence of conflicting jurisdictions between ministries: Government ministries are built to operate in silos and yet often have highly interrelated or even overlapping mandates. For example, more than 50 percent of Sub-Saharan African countries and over 70 percent of West and Central African countries’ education systems are represented by two to four ministries, representing a challenge in establishing integrated goals and policies that will allow them to reach Sustainable Development Goal 4 (Neyestani-Hailu & Reuge, 2018).
Some ministers and other government officials are unwilling to relinquish and share power over decision-making and agenda-setting processes: Ministerial commitment is paramount to effective collaboration. However, many inter-ministerial initiatives exist within the context of other competitive political and financial forces. Ministers must be on board to sacrifice some amount of independent control for collective gain.
Lack of clearly operationalized collaboration plans: Collaboration in theory is insufficient. Ministers must agree to clear lines of accountability, communication routines, and chains of implementation at the outset of collaboration.
2. HOW TO COLLABORATE? APPLIED EXAMPLES OF INTER-MINISTERIAL COLLABORATION
“Public sector performance is fundamentally about governments being able to deliver on their policy commitments for the benefit of their citizens… However, many countries adopt sensible policies that do not result in better healthcare, education, sanitation, infrastructure management or reduced crime… Improving public sector performance therefore entails closing [implementation] gaps.”
-2018 World Bank Report on Public Sector Performance
Once ministers have the intention to collaborate, they must ensure that they have a plan to do so. Just as “policy without implementation is worse than no policy at all,” the intention to collaborate without a plan to operationalize it can actually obstruct progress (Majumdar, 2006). Thus, in order to effectively implement a collaborative initiative, ministers should clearly identify the following for each participating ministry:
Programmatic Role: What programs and/or elements of the collaborative initiative is this minister and ministry responsible for implementing? What are the key actions that they will take to do so? What is the timeline associated with each of these key actions?
Political Role: How can this minister and ministry use their political capital to support the collaborative initiative? How can they generate support with the President and/or Prime Minister, other ministers, constituents, and other stakeholders?
Collaborative Role: What is this minister and ministry’s role in communicating, liaising, holding others accountable to support effective collaboration? Who is the lead ministry? What lines of accountability will be drawn between ministries and what communication routines are expected? What is the chain of implementation?
Budgetary Information: How will fiscal space be created to support the cost of this collaborative initiative?
This section includes examples of collaborative initiatives that showcase collaboration at different levels of commitment and scale, examine how each initiative was operationalized, and the pitfalls and successes that resulted. Table 4 highlights where these case studies appear within the spectrum of scale and commitment.
Table 4. Case Studies in Inter-Ministerial Collaboration
Scale
Examples
Whole-of-Government
A. Moldova
B. Ethiopia
Sectoral
C. Brazil
Bilateral
D. Kenya
A. Collaborating to Improve the Livelihoods and Promote the Rights of Persons with Disabilities in Moldova
Ministries/Agencies Involved:
Ministry of Education
National Bureau of Statistics
Ministry of Labor, Social Protection and Family
Ministry of Health
Programmatic, Political, and Collaborative Roles:
Ministry/Agency
Role
Ministry of Education
Prioritized funding of project; Code of Education modified to be more inclusive of students with disabilities; national curriculum on inclusive education created and used to train hundreds of teachers.
National Bureau of Statistics
Began measuring information related to inclusive education and reformed their data collection process to promote accurate monitoring of project progress.
Ministry of Labor, Social Protection and Family
Worked with organizations representing persons living with mental disabilities to reintegrate unnecessarily institutionalized persons back into their communities.
Ministry of Health
During the writing and implementation of a national health initiative, ensured that community mental health centers were established in every district of the country.
Budgetary Information:
The Ministry of Education prioritized funding intended to ensure children with disabilities had access to mainstream education services; supplemented with international funding.
Successes:
Reduced traditionally siloed nature of ministries.
Collective strategy was carefully designed before the intervention began.
Society’s understanding of the rights of persons with disabilities increased.
The project planning teams involved persons who would be affected by its implementation.
Capacity of local health authorities increased.
Judges’ understanding of legal rights of persons with mental disabilities improved.
New admissions to mental health institutions were reduced and there was an increase in the reintegration of former institution residents into original communities.
Pitfalls:
Collaboration limited to singular funding proposal, not institutionalized to support future collaborative efforts.
From 2005 to 2015, the number of citizens with disabilities in Moldova had increased by 20% (UNDG, 2015). Access and quality of treatment for those with mental and intellectual disabilities was of particular concern for the government, as they are some of the most common types of disability in Moldova and these persons “are more vulnerable to exploitation, violence, and abuse and other losses of human rights” (UNDG, 2015). A welcome invitation arrived in 2012 when the government of Moldova was encouraged to submit plans for funding aimed at advancing the rights of its citizens with disabilities to the UN Partnership to Promote the Rights of Persons with Disabilities (UNPRPD). Leaders created a plan that involved the high-level collaboration of many segments of the Moldovan government which was eventually accepted and, following financial and logistical support from the UN, implementation began in January 2013 (UNDG, 2015).
Moldova’s national campaign to improve the standard of living for their citizens with disabilities utilized the whole-of-government approach. The plan submitted to the UN required that ministers and leaders of national bodies reform their respective areas of the government in a collective march towards a society more inclusive and informed of disability rights. Three of the core goals of the plan were to increase the capacity of city and regional authorities to support Moldovans with disabilities locally, deinstitutionalize persons whose disabilities did not require hospitalization, and increase the inclusivity of education systems. Each ministry had clearly defined responsibilities for implementation within their sector. The Ministry of Education developed a new national curriculum that emphasized inclusivity, taught practitioners how to effectively instruct all types of students, and ensured that their schools were inclusive. With the goal of accurately monitoring the implementation of inclusive practices in schools, the National Bureau of Statistics began to measure information related to inclusive education and reformed the framework related to their data collection process. The Ministry of Labor, Social Protection and Family introduced the National Strategy and Action Plan on Adult Deinstitutionalization to ensure that mental healthcare became covered under primary healthcare plans and that community health centers were opened in every region of Moldova. Finally, the Ministry of Health created the National Mental Health Programme, a nationwide medical strategy that resulted in the opening of community mental health centers in all districts of Moldova starting in January 2014.
B. Collaborating under the Seqota Declaration to Eliminate Stunting in Ethiopia
Ministries/Agencies Involved:
Ministry of Health
Ministry of Agriculture and Natural Resources
Ministry of Livestock and Fisheries
Ministry of Water, Irrigation, and Energy
Ministry of Education
Ministry of Labor and Social Affairs
Programmatic, Political, and Collaborative Roles:
Ministry/Agency
Role
Ministry of Health
Lead ministry; brought on board Deputy Prime Minister and Regional Presidents of critical regions to show support; improved delivery of direct nutrition interventions through the public health system; improved WaSH education and behavior.
Ministry of Agriculture and Natural Resources
Increased production and consumption of locally available, nutrient-dense crops; co-chair coordinated multisectoral committees.
Ministry of Livestock and Fisheries
Increased small-scale livestock ownership.
Ministry of Water, Irrigation, and Energy
Expanded irrigation potential to improve water-use efficiency and extend growing seasons; improved quality and increased quantity of water in households, health facilities, and schools; improved access to hygienic sanitation facilities.
Ministry of Education
Included school health and nutrition strategies in education programs to improve related services for school-age children; co-chair coordinated multisectoral committees.
Ministry of Labor and Social Affairs
Expanded existing social safety net program to improve child protection, women’s empowerment, gender equity, and economic access.
Budgetary Information:
Despite limited initial funds, strong guidance and commitment by government leaders effectively developed political will and led to increased financial investment; supported by international funding.
Successes:
Leaders’ effective use of political pressure yielded funding from donors that would otherwise not have been available.
Reduced traditionally siloed nature of ministries.
Clear organizational structure for collaboration.
Pitfalls:
Weak accountability between collaborating ministries.
Effectiveness of coordination varies at regional levels of government.
Ethiopia has long identified stunting as a serious, intersectoral concern impeding its human capital development efforts. Children who are stunted have, on average, lower academic performance, reduced wages as adults, and a potentially heightened risk of nutrition-related chronic illnesses later in life (WHO, n.d.). Early efforts to collaborate with regards to nutrition led to the development of the National Nutrition Coordinating Body (NNCB) and the National Nutrition Technical Committee (NNTC) as part of the National Nutrition Program I (NNP I, 2008-2015) (HMLP, 2019). The NNCB involves 13 government sectors and is led by the Minister of Health with the Ministers of Agriculture and Education as co-chairs. It meets every six months and develops an annual work plan to ensure that various sectors are mainstreaming nutrition activities into detailed sector-specific plans, allocating budget to nutrition interventions, and assigning focal persons to work on nutrition. The NNTC, which also involves 13 government sectors and nongovernmental stakeholders, has three steering committees on program management, food fortification, and monitoring and evaluation. These two national entities have different goals as the NNCB is responsible for providing policy and strategic decisions related to the NNP. However, the NNTC works under the NNCB, and is responsible for the technical work related to the federal level NNP coordination. At the regional level, there is a similar structure, known as the RNCB and RNTC.
Multisectoral coordination as part of the NNPI was able to demonstrate some improvement in outcomes, but was not fully effective in creating the intended outcomes. Interventions in agriculture, health, and other sectors were not properly contextualized and everyone in government acted separately without keeping an eye on what was actually necessary to get the job done. The Minister of Health knew that incorporating nutrition goals and actions into existing programs across sectors could enhance said programs’ nutrition sensitivity and thus their likelihood of improving nutrition outcomes. Thus, in July 2015, the government initiated the Seqota Declaration, a high-level whole-of-government commitment to end stunting in children under two years by 2030. The Declaration was accompanied by the launch of the National Nutrition Program II (NNP II, 2016-2020) and the National Nutrition-Sensitive Agriculture Strategy (2016-2020). The Seqota Declaration builds on and supports the implementation of NNP II which highlights the “Five Building Blocks of Effective Nutrition Governance” as consensus building and coordination, political commitment, financing, service delivery capacity, and transparency and accountability (HMLP, 2019).
The Seqota Declaration has ten multisectoral strategic objectives and is implemented by six federal sectors (Ministry of Health; Ministry of Agriculture; Ministry of Water, Irrigation and Energy; Minister of Labor and Social Affairs; Ministry of Education; Ministry of Women, Youth, and Children). In addition to these six ministries, development partners and community organizations are also involved. To ensure stakeholders were correctly envisioning collaboration in practice, they adopted a clear collaboration framework known as the “Three Ones” which meant that there was “one goal, one plan, and one monitoring and evaluation system” in place for better coordination across sectors (HMLP, 2019). The “Three Ones” collaboration framework dictates that all nutrition-related monitoring and evaluation activities be assessed under one integrated and unified system. The different sectors involved in the Seqota Declaration each have a list of key performance indicators for which they are responsible. These indicators cut across sectors where relevant. For example, key WaSH indicators illustrated that the MOH needed to more effectively promote hygiene and sanitation practices by collaborating with the MOE during targeted interventions at school. Routine service and administrative records collected through sectoral information systems were used to provide information for timely monitoring, supervisory visits, and review meetings. Currently, the FMOH and UNICEF are working together on a pilot Unified Nutrition Information System (UNISE), a performance management tool that allows all sectors and partners to upload their targets and results so as to generate scorecards at the federal, regional, zonal, and woreda levels. This unified system is extremely important for progress towards meeting Seqota Declaration goals as it facilitates robust and continuous nutrition data management and becomes useful when seeking further investment.
In the past, there had been concerns about issues related to the bureaucracy of government, which limited intersectoral coordination mechanisms to exist only horizontally at federal and regional levels. In order to achieve the goals of the Seqota Declaration, it was necessary to establish entities with people from different sectors that would be fully dedicated to the initiative. These entities were realized with the creation of three Program Delivery Units (PDUs), a tangible “embodiment of intersectoral government” (HMLP, 2019). PDUs are small teams of multisectoral experts placed in the federal, Amhara, and Tigray President’s offices to secure higher-level political commitment to regional nutrition activities, to ensure accountability to the highest level of the regional government, and to provide technical leadership and performance management support.
Approximately two years into the implementation of NNP II and the Seqota Declaration, it is clear that the NNCB has played an important role in bringing together various ministries. However, ongoing challenges with accountability and ownership continue – there is a persistent perception that nutrition is primarily a Ministry of Health issue and a lack of accountability across ministries represents a barrier to successful multisectoral coordination. Even as nutrition has grown in national importance and public awareness, ministry staff feel that with no cross-ministry reporting structures, there has been a lack of ownership and clarity about responsibilities for nutrition outcomes. A key component of accountability is the clear delineation of roles and responsibilities for all stakeholders. However, defining a role for each sector is a challenge when it comes to nutrition: Deciding where the work of one ministry starts and ends and how it interfaces with other ministries at the national, regional, and local levels is a dynamic process with implications for political interests, leadership, budgeting, and accountability.
C. Collaborating under Criança Feliz to Improve Early Childhood Development in Brazil
Ministries/Agencies Involved:
Ministry of Citizenship
Ministry of Education
Ministry of Human Rights and Culture
Ministry of Health
Programmatic, Political, and Collaborative Roles:
Ministry/Agency
Role
Ministry of Citizenship
Lead ministry; coordinated efforts through Secretariat for Promotion of Human Development; established home-visiting budget.
Ministry of Education
Accommodated children found to have learning disabilities during home visits.
Ministry of Human Rights and Culture
Ensured that home visits under the program included culturally relevant activities for all children.
Ministry of Health
Improved the health conditions of children found to be ill during home visits.
Budgetary Information:
Each ministry contributed financially to the program; the National Management Committee, the main coordinating agency, determined the overall funding that the inter-ministerial team would allocate to the program; the Ministry of Social Development determined the home-visiting budget.
Successes:
Led by a passionate and persistent minister.
Scientific evidence supported the initiative.
Civil society coalition organized as a formal network.
Parliamentary coalition with representatives from all political groups was formed.
Shared management structures were constructed.
Implemented by a coordinating body comprised of diverse stakeholders.
Pitfalls:
On-the-ground implementation was highly variable due to unreliable levels of local preparation.
Some families resisted this new program fearing they would lose benefits from existing social programs.
In October 2016, Brazil had 15 million children under the age of four and high rates of poverty (HMLP, 2019). Economic progress had been made through cash transfer programs, but they were not enough to break the cycle of poverty and overcome the long-term challenges of violence in the country. Thus, Brazil’s Ministry of Social and Agrarian Development (now Ministry of Citizenship) introduced a collaborative early childhood development intervention called the Criança Feliz Program (PCF). PCF is a program that involves regular home visitations as the basis for multisectoral support of early childhood development. Primeira Infancia Melhor (PIM), a predecessor program to PCF, established the expectation that the division of ministry roles during home visits be widely recognized. For example, the discovery of a medical issue would require the Ministry of Health to act; the presence of a child with a learning disability automatically prompts action from the Ministry of Education; the Ministry of Human Rights and Culture is obliged to ensure that the government visitors brought culturally appropriate materials with them to the homes.
The introduction of PCF was only possible due to the significant groundwork laid by Minister of Citizenship Osmar Terra that established early childhood care as a national priority: Minister Terra launched a cross-sector alliance of child advocacy stakeholders in 2003, formed another far-reaching coalition in 2007 that united actors from across government ministries, civil society organizations, and businesses, and later led the charge to create a collection of representatives from ministries that sought to enact a federal law instituting a national legal framework guaranteeing the rights of children across varying public policy domains. PCF began as a direct consequence of this federal law.
The Ministry of Citizenship coordinates the efforts through the Secretariat for the Promotion of Human Development and management committees exist at the national, state, and municipal levels. The National Management Committee houses representatives from the Ministries of Education, Health, Human Rights, Culture and Social Development in what they call the “inter-ministerial government space” (HMLP, 2019). This is a place in which all involved parties have previously agreed to uphold the mission of implementing PCF; as a result, it serves as a place to coordinate and solve technical issues, rather than argue about objectives. This intersectoral committee was created by presidential decree, giving it the formality and gravitas to ensure that each ministry prioritizes it appropriately. The management committee has high-level representation from each ministry, and it is therefore a place for decision-making, rather than day-to-day collaboration. To get things done, there is also the Technical Group, under which a number of inter-ministerial working groups coordinate efforts.
An example of collaboration that has been achieved by the Technical Group and the National Management Committee is the redesign of the notebook that mothers receive after they give birth. Traditionally, the Ministry of Health would provide such mothers a notebook that included general child health tips. Now, since the creation of the National Management Committee, these notebooks include information about child development milestones and cultural specificities contributed by other ministries. Other examples of collaboration include a guide for visitors for children with disabilities and the development of training materials and workshops for both visitors and families.
The general duties of the National Management Committee are to strengthen the intersectionality of the program, to approve training and program resources, to make decisions about the stages of the program, and to agree on regulatory instruments that distribute responsibilities for different policies. One especially important responsibility, though, is to set the intersectoral budget.
As coordinator of the program, the Ministry of Citizenship sets the home-visiting budget, which it distributes to the municipalities through the National Fund of Social Assistance. Its leaders decided to organize this fund so that the resources would flow directly from the ministry to each municipality, avoiding intermediaries and countless individual contracts. However, a budget for home-visiting is inadequate to ensure the success of PCF. It was important that each ministry allocate funds in order to effectively address the intersectoral needs that emerge from the visits. The National Management Committee is the place where the ministries negotiate the allocations that each ministry will contribute to PCF.
At the state level, similar Management Committees exist, but are composed of representatives from State Secretariats. The role of Secretariats is to monitor the implementation and to give technical assistance to the municipalities. To achieve this goal, Secretariats hire multiplicadores, professionals who are educated by national-level trainers. In turn, they go on to train local coordinators, who train local visitors. This modality of waterfall training has led to a number of implementation problems; however, it was the only way that Brazil could scale the program to over 2,000 municipalities in just one and a half years.
At the municipal level, Municipal Management Committees are much more operational in scope. They discuss, support, and approve operational issues of the program. For instance, they identify the beneficiaries of home visits, hire and organize local training for visitors, follow up with different sectoral responses on the demands that they identify, and coordinate with local NGO networks. At the municipal level, intersectoral collaboration is often informal and they escalate any challenges to the state level.
A final component of Brazil’s inter-ministerial implementation effort is its integrated information system, Cadastro Único, which allows different ministries to identify families and work from the same data. This has been an important tool because without it, the registries of potential beneficiaries housed by each ministry would vary, thereby leading to coordination problems and leaving people unattended. This has also allowed for more effective monitoring and evaluation of implementation across ministries.
Today, after almost three years, PCF has survived a change of president in Brazil and it grows day by day as more and more municipalities voluntarily sign up for the program. To date, PCF has made it possible for nearly 500,000 children and 85,000 pregnant women in Brazil to receive home visits every week, a total of almost 2.4 million visits a month in over 2,000 municipalities (HMLP, 2019).
D. Collaborating Through a Zoonotic Disease Unit (ZDU) to Improve Public Health Outcomes in Kenya
Ministries/Agencies Involved:
Ministry of Health
Ministry of Agriculture, Livestock and Fisheries
Programmatic, Political, and Collaborative Roles:
Ministry/Agency
Role
Ministry of Health
Contributed one medical epidemiologist to ZDU; created and supported county-level One Health teams; advocated for and coordinated funding.
Ministry of Agriculture, Livestock and Fisheries
Contributed one veterinary epidemiologist to ZDU; created and supported county-level One Health teams; advocated for and coordinated funding.
Budgetary Information:
Each ministry contributed financially to the ZDU and supplemented ZDU funds by engaging multilateral and bilateral agencies and partners, local and international research institutions and universities working on zoonosis in Kenya.
Successes:
Reduced traditionally siloed nature of ministries and sectors.
Strengthened capacity for surveillance and reporting in the animal health sector.
Foundation of effective national coordinating office.
Pitfalls:
Implementation gaps continued at the local level.
Unequal financial capacity of participating ministries prevented full realization of plan.
Change in government structure required modification of strategy.
A recent global movement called One Health recognizes the connection between the health of people, animals, and the environment and seeks to employ a collaborative, multisectoral approach to achieve improved outcomes for each. Kenya is one country that utilizes the One Health approach. On August 2, 2011, the Ministry of Health (MoH) and Ministry of Agriculture, Livestock and Fisheries (MALF) signed a Memorandum of Understanding agreeing to collaborate by jointly administering the ZDU (Republic of Kenya, 2014). The ideal structure and mission of the ZDU was investigated and debated for four years before being finalized and the divide in power and responsibility between ministries was clearly specified before the collaboration began. The MoH and MALF maintain equal authority over the ZDU, each contributing financially and periodically staffing the unit with one senior epidemiologist who ultimately returns to their respective ministry to report updates (Republic of Kenya, 2014; Mbabu et. al, 2014). Through the ZDU, the ministries co-author human and animal health studies, create and support county-level One Health teams, and advocate for and coordinate funding (Mwatondo et al., 2017). The national One Health coordination office was tasked with improving the prevention, monitoring, and control of zoonotic epidemics. While the ZDU is primarily a bilateral approach to collaboration, the team is empowered to collaborate with experts affiliated with both government and private sectors from veterinary health, public health, wildlife health, and information communication and technology, among others.
Relatedly, forward-looking changes were made to the education and on-the-job training of veterinary and medical fields. Since 2004, veterinarian and medical students have had the option to lead teams comprised of both fields through a zoonotic outbreak investigation as part of their training in order to develop a One Health-ready workforce (Mwatondo et al., 2017). This joint training approach has removed long-standing boundaries between the education systems and replaced them with collective networks. This collaboration continues into their professional lives, when medical specialists from the MoH and veterinary specialists from the MALF are trained in unison, allowing members from each ministry to acquire a deep understanding of the other (Munyua et al., 2019).
Since its foundation, the ZDU and its partners have discovered new pathogens key to improving readiness for zoonotic disease prevention; widened and improved national programming that increases public awareness of zoonotic disease prevention; developed and updated evidence-based prioritization of zoonotic diseases critical to public safety; incorporated the reporting of zoonotic diseases into the general disease surveillance system, ensuring prioritized zoonotic diseases are no longer neglected; and developed the Strategic Plan for the Elimination of Human Rabies in Kenya 2014-2030 (Munyua et al., 2019; Octaria et al., 2018).
3. SUCCESSFUL TAKEAWAYS: A DECISION-MAKING GUIDE
This section synthesizes the previous information into a decision-making manual that can guide policymakers through the process of launching collaborative efforts across ministries.
Determining the Optimal Level of Commitment
Collaboration between ministers spans a spectrum of commitment ranging from the informal to the formal. The characteristics of a given intervention that spurs inter-ministerial collaboration can provide helpful insight into determining the ideal level of commitment for that endeavor.
Leaders of an intervention would want to advocate for informal collaboration if:
The intervention involves short-term goals (Majumdar, 2006).
The intervention would be better supported by the occasional sharing of information or sharing of limited resources because the initial process of completely intertwining budgets and/or significant resources would be too time-consuming relative to the goals.
Existing collaboration between stakeholders is weak or nonexistent and it seems unlikely that coordination will be mandated by law anytime soon.
Alternatively, an intervention should be coordinated and implemented through formal inter-ministerial collaboration if:
The intervention seeks to generate substantial, long-term change (Majumdar, 2006).
The intervention would benefit from deeply connected budgets and in-depth deliberation on every aspect of the process and has the initial time to devote to this process.
The political will exists to enshrine collaborative principles between stakeholders in law.
Determining the Optimal Level of Scale
Inter-ministerial collaboration can occur between two ministries (bilateral), three or more ministries of related focus (sectoral), or involve all or most government ministries (whole-of-government). When concluding which of these three avenues of scale is most appropriate for a given collaboration, it is most important to consider the number, demographics, and needs of the targeted constituents. Consider the following examples:
Bilateral collaboration: The Ministry of Veterans Affairs is interested in improving the lives of military service members after the conclusion of their service. It has been determined that by far the most pressing challenge for former military service members is meeting the expected qualifications of new jobs as they transition into new sectors. Thus, increasing the accessibility and quality of veteran job training programs will be the primary focus of their intervention. As this is a specific group of citizens and a single issue has been identified as the focus, the Minister of Veteran Affairs has decided to collaborate with the Ministry of Labor under a bilateral agreement to carry out this intervention.
Sectoral collaboration: The Ministry of Housing is attempting to drastically reduce the rate of homelessness among youth in its country. Upon examination, it becomes clear that the housing status of parents (and subsequently their youth) is strongly associated with the level to which parents have access to quality education and healthcare. Realizing that providing housing to homeless youth will require dedicated support from these related sectors, the Ministry of Housing enlists the Ministry of Education and the Ministry of Health to develop a plan and collaborate throughout its implementation.
Whole-of-government collaboration: A Prime Minister is dedicated to reforming the way in which their country consumes energy. They have pushed for and achieved the passing of legislation that requires every ministry to submit a plan for approval that demonstrates how they will shift their operations to be run on primarily green energies by 2030. The Prime Minister and each ministry head then collaborate to develop best practices and reasonable benchmarks, collectively reassessing progress every six months and making changes when necessary.
Enabling Factors for Successful Inter-Ministerial Collaboration
Existence of strong and sustained political leadership: The preliminary political backing of at least one senior official is vital to launching and sustaining collaborative efforts. If such an official is not involved, stakeholders interested in installing a collaborative intervention should prioritize enlisting one. The government leader should be “technically skilled and politically savvy, as well as close to the chief executive” and should be adept at forming and maintaining productive relationships (UNDG, 2015).
Detailed, inclusive planning occurred before implementation: Inter-ministerial interventions operate with shared elements of responsibility and accountability, and any lapse in understanding of the daily objectives or overall mission threatens to derail the efficacy of the initiative. One effective way to prevent such lapses is to develop robust collaboration plans that clearly outline roles, routines, and the chain of implementation.
Significant emphasis placed on the creation of buy-in and changing of culture: It is likely that there will always be some level of pushback when collaboration begins. Collaborative efforts that were most successful anticipated this and responded by uniting the curriculum of students who will eventually support the intervention, hosting communal training sessions of stakeholders, and soliciting the assistance of top-level leaders (UNDG, 2015).
Coordinating offices established at different regional levels: Particularly when an intervention requires collaboration across significant geographic boundaries, the installment of coordinating offices across a country at regional and municipal levels is helpful in ensuring constant and clear communication between stakeholders and supporting downstream implementation of collaborative efforts.
References
Colgan, A., Kennedy, L., & Doherty, N. (2014). A primer on implementing whole of government approaches. Centre for Effective Services. Retrieved from: https://bit.ly/31KWdKU
Dill, D. & Kopsick, D. (2017). Improving cooperation between customs and environmental agencies to prevent illegal transboundary shipments of hazardous waste. World Customs Journal, 8(2). Retrieved from: https://bit.ly/2MSTH11
Majumdar, D. (2006). Collaboration among government agencies with special reference to New Zealand. New Zealand Ministry of Social Development. Retrieved from: https://bit.ly/2BMD4NZ
Mbabu, M., Njeru, I., File, S., Osoro, E., Kiambi, S., Bitek, A., … Njenga, K. (2014). Establishing a one Health office in Kenya. The Pan African Medical Journal. Retrieved from: https://bit.ly/31SfJVC
Munyua, P., Njenga, M., Osoro, E., Onyango, C., Bitek, A., Mwatondo, A., … Widdowson, M. (2019). Successes and challenges of the one health approach in Kenya over the last decade. BMC Public Health, 19(3). Retrieved from: https://bit.ly/2pj6NLY
Mwatondo, A., Munyua, P., Gura, Z., Muturi, M., Osoro, E., Obonyo, M., … Thumbi, S.M. (2017). Catalysts for implementation of one health in Kenya. The Pan African Medical Journal. Retrieved from: https://bit.ly/36kIZYS
Neyestani-Hailu, L. & Reuge, N. (2018). Strengthening national learning systems towards SDG4-Education 2030 and CESA. RCG4 Education Systems Strengthening Task Team. Retrieved from: https://bit.ly/346q95F
Octaria, R., Salyer, S., Blanton, J., Pieracci, E., Munyua, P., Millien, M., Nel, L., & Wallace, R. (2018). From recognition to action: A strategic approach to foster sustainable collaborations for rabies elimination. PLOS Neglected Tropical Diseases. Available at: https://bit.ly/2NlUnLa
Harvard Ministerial Leadership Program. (2019). Intersectoral collaboration in the Criança Feliz early childhood intervention program.
Republic of Kenya, 2014. National Strategic Plan for the Implementation of One Health in Kenya. Available at: https://bit.ly/33ZBNPQ
Roberts, J. & O’Connor, P. (2007). The inter-agency services collaboration project. Wellesley Institute. Retrieved from: https://bit.ly/2pTDEqK
UN Development Group, 2015. Eight Case Studies on Integrating the United Nations’ Normative and Operational Work. Available at: https://bit.ly/2PpQqIe
Wanna, J. (2008). Collaboration government: Meanings, dimensions, drivers and outcomes. Australian National University. Retrieved from: https://bit.ly/31SOYkb
World Bank, 2018. Improving Public Sector Performance: Through Innovation and Inter-Agency Coordination. Available at: https://bit.ly/2PmWv8c
World Health Organization, n.d. Stunting in a Nutshell. Available at: https://bit.ly/346prW8
Nicholas Masada, Ed.M.,
Harvard Graduate School of Education
The Program for Education, Health and Nutrition (PROGRESA) was established in 1997 as a response to the political and economic crisis that unraveled Mexico in 1994. It aimed to improve the wellbeing of families through the increase in consumption capacity and the creation of human capital to break the intergenerational poverty cycle. Studies and evaluation on the program have shown its relevant impact in improving access to health services, nutritional benefits and the education status of Mexico’s poorest populations. The program provided cash transfers1 directly to poor families under three conditions:
School attendance for children between third year of primary and third year of secondary (with higher subsidies provided to households with girls).
Utilization of a package of preventive health interventions, health educational talks and provision of diet supplements for children and pregnant women.
Participation in health consultations and educational sessions.i
In 2002, in addition to its original components, the program widened its benefits to include factorsii such as:
Educational scholarships for children
Money for school supplies
Additional support for households with elderly members over 70
Medical services and health education
Savings accounts for youth who finish secondary school
Support for household energy consumption
The most recent expansion of the program under the name of Prospera aimed to promote access to higher education and formal employment opportunities to its beneficiaries. Additionally, Prospera strived to increase access to financial services and foster increased social inclusion to the poorest citizens.iii Federal administrations have changed the program’s name throughout its period, though its basic structure remained the same. It was initially called Progresa (1997-2001), then Oportunidades (2002-2012) and, finally, Prospera (2012-2018) (referred to as P-O-P). The Mexican model of a conditional cash transfer (CCT) program has been replicated in more than 50 countries across Latin America, Africa and Asia.
1Equivalent to one-third of their household income.
Program Impact
Impact on Poverty Alleviation
The program has achieved notable results in helping to alleviate poverty throughout Mexico. P-O-P substantially improved the household income distribution in the country as well as strengthened other poverty indicators. Evaluations showed that expanding the program significantly reduced the poverty rate by 1.8 percentage pointsiv. Figure 1 shows the decreasing trend in the poverty headcount ratio from the mid-1990s. Other indicators such as poverty incidence, poverty severity and inequality decreased dramatically due to the programv.
The program also helped in increasing overall labor participation, especially for women. Labor market effects that were found included an increase in women’s profitability from working, a rise in the total number of work hours per woman and improvements in women’s labor earningsvi. Additionally, the program led to higher paying jobs for men as well as gains in employment benefits such as health insurancevii.
Improvements in Health
Evaluations of P-O-P showed that the program “increased the number of antenatal care visits, reduced infant mortality rates and improved postnatal care provided by trained personnelviii”. Due to program efforts, P-O-P beneficiaries received 12% more prenatal proceduresix and utilized public clinics more than non-beneficiariesx. Due to increased visits and less frequent illnesses, there was a reduced demand for curative care and a decrease in the number of hospital inpatient stays. The health effects also proved strongly positive among children. The incidence of illness among children in recipient households diminished by nearly 23 percent. Children also recorded a reduced rate of anemia and an increased percentage in heightxi.
Increased Access to Education
The program conditions resulted in direct educational attainment benefits in Mexico. An analysis on the program’s educational components found significant effects on student learning, particularly among indigenous childrenxii. There was also increased enrollment at the telesecondary and high school levels, especially for young girlsxiii. Younger children who benefitted from P-O-P were also found to be less likely to repeat a grade and more likely to progress to the next gradexiv. The program was also shown to reduce school dropouts and encourage reentry among those who were out of school.
Key Factors of Success
Coordination Across Ministries
The coordination of P-O-P was administered by a deconcentrated unit from the Ministry of Social Development (SEDESOL) responsible for the program’s execution. Most decisions were taken at the national level, but offices were opened in the states to coordinate daily operations and establish relationships with the states. The central level also had a National Technical Council and National Technical Committee which consisted of representatives of SEDESOL as well as Ministries of Financing, Public Education, Health and Social Security.
Though the program was under the administration of SEDESOL, its origin is accredited to the policy efforts of the Ministry of Finance, particularly with former Deputy Finance Minister Santiago Levy being the architect of the programxv. Once the administration implemented Levy’s report on poverty alleviation, it increased “funding to be allocated to state governments for distribution to municipalitiesxvi” and executed a successful pilot program. Based on initial observations of the pilot program, the former deputy finance minister advocated for better monitoring and increased interagency coordination before the scaling of the programxvii.
P-O-P represented a significant paradigmatic change in the development of anti-poverty programs which implied not only the creation of the program, but the transformation and cancellation of existing programs and institutions, the creation and strengthening of others, as well as reallocation of public budget. The comprehensive approach, with each ministry having a ‘stake’ in the program’s success, has been attributed as one of the factors that helped the program survive through changes in administrationxviii.
Evaluation Project
For the first time in Mexico, the government incorporated an ambitious, long-term impact evaluation project during the rollout of the CCT program. This component has played a vital role in constructing evaluating practices and institutions in Mexico over the last few decadesxix. The rigorous evaluation approach emphasizes the need for clear data to measure effectiveness and ensure the program could adapt through political changesxx.
Since evaluation was prioritized from the beginning, evaluators were able to collect baseline data used to construct quasi-experimental designs. The positive results of the evaluation project have helped in obtaining support for the expansion of the program. Progresa has been heralded as “one of the few poverty-reduction programs that has been able to prove its impactxxi”.
Finance Mechanisms
One of the key decisions made by the Mexican government during the beginning of the program was to gradually reallocate food subsidies that had previously been ineffective towards Prosperaxxii. This not only re-designated funds that were being used inefficiently but also helped diminish additional pressures on the federal budget.
The program began with an initial coverage of 300,000 families and a budget of $58 million (USD)xxiii, accounting for 0.004% of the country’s GDP. The budget was progressively raised over a decade to represent 0.47% of GDP in 2016. While P-O-P was one of many programs in the state policy against poverty, it was the program that concentrated the highest budget. In 1997, it represented 1.67% of the overall budget of anti-poverty programs and, by 2017, reached 21.3%. These numbers demonstrate that P-O-P represented a key program in the social policy by dominating one-fifth of the total budget allocated to combat poverty in Mexicoxxiv.
Challenges
Targeting
P-O-P used geographical and household targeting to maximize efficiency in its allocation of resources to the poorxxv. The underlying design of this approach resulted in high, unexpected targeting errors that left an extensive proportion of poor families uncovered by the cash transfer mechanism.
Implementation evaluations of the program showed that the “targeting mechanism failed to identify households with a small number of members or households without young childrenxxvi.” It has been estimated that 24% of those who qualified were not covered and 22% of those who were not qualified received coveragexxvii. The program’s focus on rural areas, particularly in places that already had school infrastructure and health services, effectively excluded the poorest with no access to public services as well as the urban poorxxviii. An attempt to correct these deficiencies was made in 2016 when poor families without access to schools and health centers were incorporated into the program. Single families received an extra budget that represented around 12% of the budget that year.
Social Tensions
The household-focused method of distribution of cash transfers led to social tensions in some communities. Since certain households received benefits while others did not, it became easy for neighbors to tell who was or was not a beneficiary of the program. In a focus group with CCT recipients, 90% of the respondents believed that the selection process was ‘unfair’ as they perceived that those who needed benefits the most seldom received themxxix. This perception of unfairness prompted “contempt, resentment or envy” within some communitiesxxx. Although these types of problems were considered important by the general coordination, the rationale of selecting families did not change over the period of P-O-P’s existence as those decisions were based on a technical rationale.
References
Gertler, Paul, and Simon Boyce. “An Experiment in Incentive-Based Welfare: The Impact of PROGESA on Health in Mexico.” Working Paper, April 2001.
IFPRI, 2011. “The Impact of Oportunidades in Mexico”. International Food Policy Research Institute.
The World Bank, 2014. “A Model from Mexico for the World”. Accessed via worldbank.org website.
Debowicz, Dario et al, 2013. “The impact of Oportunidades on human capital and income distribution in Mexico: A top-down/bottom-up approach”. Journal of Policy Modeling.
Debowicz, Dario et al, 2013. “The impact of Oportunidades on human capital and income distribution in Mexico: A top-down/bottom-up approach”. Journal of Policy Modeling.
Parker, Susan, 2018. “The long-term effects of cash transfers: Mexico’s Progresa.” VoxDev.
Parker, Susan, 2018. “The long-term effects of cash transfers: Mexico’s Progresa.” VoxDev.
Servan-Mori, Edson et al, 2019. “Improving the effective maternal-child health care coverage through synergies between supply and demand-side interventions: evidence from Mexico.” Journal of Global Health.
Barber, Sarah, 2009. “Empowering women to obtain high quality care: evidence from an evaluation of Mexico’s conditional cash transfer programme.” Journal of Health Policy Plan. National Institutes of Health.
J-PAL, 2001. “The Impact of PROGRESA on Health in Mexico”. Accessed online via povertyactionlab.org.
J-PAL, 2001. “The Impact of PROGRESA on Health in Mexico”. Accessed online via povertyactionlab.org.
World Bank. 2019. “Impacts of PROSPERA on Enrollment, School Trajectories, and Learning (Spanish)”. Policy Research working paper.
Ibid.
Behrman, Jere, 2005. “Progressing through PROGRESA: An Impact Assessment of a School Subsidy Experiment in Rural Mexico.” The University of Chicago Press Journals.
Brookings, 2020. “Brookings Institute – View All Experts.” Accessed via brookings.edu website.
Teichman, Judith, 2003. “The Politics of Freeing Markets in Latin America: Chile, Argentina, and Mexico.” University of North Carolina Press.
Bate, Peter, 2004. “The story behind Oportunidades.” The Inter-American Development Bank.
Greene, Meghan, 2012. “Extending Oportunidades: A Look into Mexico’s Model Conditional Cash Transfer Program”. Center for Financial Inclusion.
Alderman, Harold, 2018. “The 1.5 Billion People Question: Food, Vouchers or Cash Transfers?” The World Bank Group.
Greene, Meghan, 2012. “Government Steps in Youth and Finance”. Center for Financial Inclusion.
Bailey, Stephanie et al, 2007. “Conditional Cash Transfer Programs in Latin America”. University of Michigan Paper.
Nino, Miguel, 2017. “Mexico’s Progresa-Oportunidades-Prospera and the raise of social assistance in Latin America”. United Nations University.
Levy, Santiago. “Progress Against Poverty: Sustaining Mexico’s Progresa-Oportunidades Program.” Brookings Institute.
Ibid.
Adato, Michell, 2000. “The Impact of Progresa on Community Social Relationships”. International Food Policy Research Institute.
Azevedo, Viviane, 2013. “Multidimensional Targeting: Identifying Beneficiaries of Conditional Cash Transfer Programs.” Social Indicators Research.
Ibid.
Nino, Miguel, 2017. “Mexico’s Progresa-Oportunidades-Prospera and the raise of social assistance in Latin America”. United Nations University.
Adato, Michell, 2000. “The Impact of Progresa on Community Social Relationships”. International Food Policy Research Institute.
From 2002 to 2010, Colombia underwent an Educational Reform under the leadership of Minister of Education Cecilia María Vélez White, which strived to develop a more efficient system to ensure education access for all through tackling local union power and interests with firm and decisive actions (MinEducación, 2010).11 This set the foundation for profound changes that to date have resulted in increased access to educational services from early childhood (reaching 646,188 children with comprehensive attention by 2009) to higher education (63% increase from 2002 to 2009). The number of students in pre-school, primary, and middle school rose from 9,994,404 in 2002 to 11,241,474 in 2009; quality improved in K-12 where dropout rates decreased from 8% in 2002 to 5.4% in 2008 and tertiary education certification increased with the number of graduate students graduating with masters degrees growing (6,776 in 2002 to 16,317 in 2008). In addition, the reform almost tripled the number of doctorate students from 350 to 1,532 in the same period; and led to the creation of information systems for improved data collection and problem solving. As with any large-scale transformation, a number of factors had to align to create a conducive environment.
Such was the case of Colombia during the two-term presidency of Álvaro Uribe Vélez, where the intentional political and operational strategy of the administration involved many confluent stakeholders aiming together for the same objectives. It is through this lens that this case study will examine Colombia’s education revolution with the ultimate goal of highlighting actionable strategies that current ministers can employ to facilitate their own institutional change.
Legislative Environment: Tools for a Reform
To understand the success of the Educational Revolution in Colombia, one first needs to analyze the process that began a few years prior to actual policy implementation. In the early 2000s, Colombia was living through a period of great instability caused on the one hand, by an ongoing armed conflict that had eroded its social tissue and blurred the lines of the State, and on the other hand of the biggest financial crises in its recent history. With a rapidly increasing deficit, Colombia had to commit to more efficient use of the nation’s budget. As a result of these contextual factors, President Andrés Pastrana introduced two key pieces of legislation in 2002, the last year of his administration, that laid the groundwork for Colombia’s Educational Revolution.
The first piece of legislation (Law 715) modified a previously instated decentralization process that changed the way resources were allocated. It “unified the budgetary allocation and the contributions to the national government’s revenue in a General Contribution System (SGP)” (MinEduación, 2010)11 and shifted many attributions that had previously been conferred to the territories back to the national government. One of the consequences of these decentralization laws was that the implementation of educational policies was now the mandate of local Secretaries of Education. In cities where the population was greater than 100,000 citizens, new administrations were created with more ascriptions. The administration of education in rural areas also shifted from the national government and became the responsibility of the now enhanced local Secretaries of Education.
To help the President tackle the surrounding crisis, Congress authorized for extraordinary legislative powers to be attributed to the President to transform the educator’s career path. This led to the second big legislative change which had to do with the teachers’ promotion system. Previously, teacher salary raises were determined only by seniority (rather than by merit) and with increasing seniority each year, the system had become unpayable and urgent change was needed. Two different options were considered to deal with the salary situation: (1) the possibility of reforming a teaching statute seemed unlikely to find consensus among the union leaders, educator, education specialists, and the government due to the short time available, or (2) the introduction of a statute that would only be applied to new teachers entering the workforce with entrance exams and evaluation for promotion. A fast negotiation with a fragmented Teacher Union, which had internal problems due to unstable leadership and to the fact that many of its representatives in Congress were not grouped in a single front, but rather in several political parties, that doubted that the government would be able to move forward with a new proposal concluded with the introduction of a new and controversial teaching statute, the 1278 Presidential Decree (MinEducación, 2010).11
Political Context: 2002 Presidential Campaign & Selection of Minister of Education
Concurrent with these legislative changes, Colombia was in the midst of a presidential campaign. At the time, both the business community and civil society were strong proponents of the idea that education should be a central piece of a Colombia that was forward looking. Colombia’s constitution mandated that the political platform and proposal of any presidential candidate that was elected became the basis for the national strategic plan. Knowing this, some representatives of the business community and civil society organized a series of dialogues and encounters with all presidential candidates in which they talked about their vision for the education sector moving forward. It was clear that stability was crucial, since the average term in office of a Minister of Education in Colombia had historically been only seven months. During these encounters, representatives from the sectors conveyed to all candidates that for a meaningful change in the education sector to take place, it was necessary for them to name a Minister that would stay in their position for the full length of the administration.
The presidential campaign saw the rise of a local politician whom many perceived as an outsider: Álvaro Uribe Vélez. He had won his nomination as an independent candidate without the formal support of a political party, and a strong stance against the FARC (Colombian Revolutionary Armed Forces). Uribe promised the business community and civil society that if he won, he would only name one Minister of Education for the full length of his administration. He ultimately won the presidency with over 53% of the vote and his allies won Congress in a landslide.
With presidential victory in hand, Uribe began his search for the ideal person to become the next Minister of Education. Cecilia María Vélez White emerged as the natural candidate. Minister Vélez had majored in Economics at the Louvain University in Belgium and pursued graduate studies in urbanization at Massachusetts Institute of Technology. Her experience at the Central Bank, the Ministry of Foreign Affairs, and the National Planning Department provided her with insights into both public administration and finances.
Vélez was a well-respected name in the sector due to the profound change she had achieved as Secretary of Education in Bogotá (1998 – 2002) during the government of Mayor Enrique Peñalosa, which continued with Mayor Antanas Mockus. During her time as Secretary, her team had been at the forefront of the decentralization process from a local administration perspective and had the opportunity to “pilot” some of the changes she would later implement at a national scale. She was able to create information systems to more accurately collect data on student enrollment, teacher attendance, and infrastructure tracking. She used this data to track school performance, identify infrastructure needs, and adjust teacher pay based on absenteeism. The results of her ministry’s interventions could be clearly seen in non-profit public education providers that operated in highly marginalized neighborhoods, known as Concession Schools. These schools saw improvements not only in standardized test scores but also in process indicators such as parent participation and school punctuality, which could be easily contrasted with those of nearby public schools who did not receive the same interventions.
In her role as Secretary, Vélez acquired an insightful perspective into the education sector and learned some of the strategies to negotiate with different stakeholders. Her management style and professionalism helped her consolidate a high-quality technical team that would continue with her throughout the years as Minister.
Given her track record of success in both leadership and implementation, President Uribe invited Vélez to become Minister of Education. While the emphasis of President Uribe’s administration was security and stabilizing the country, he was still a strong proponent of Minister Vélez and her education reform efforts for two reasons. Firstly, he was trying to regain spaces where the presence of the State had been lost and basic services had been impossible to provide due to the armed conflict. Secondly, his own management style was similar to that of Minister Vélez and thus they were able to work together easily. Thus, Minister Vélez began her term backed by a President with a very high approval rating who also had the cooperation of the majority of local authorities. This gave her significant political capital which eased the future implementation of the reform.
Leadership: Decisive Actions to Set Course
Minister Vélez came into her position with clear knowledge of the education sector and a vision to transform it. She knew she had to aspire to an ambitious set of goals that comprehensively shifted every aspect of the sector so she created a strategic plan with three main goals: to increase access, to improve quality, and to modernize institutions with the use of information systems. These goals were chosen to promote a robust system with higher standards to ensure a developed, egalitarian, and peaceful Colombia. The first period’s goal was to emphasize education as a social government policy with a strong focus on equality, and the second period would set the education policy as a cornerstone of competitiveness for the country (MinEducación, 2010).11 But to start, she first needed to “put the house in order” in her ministry.
Minister Vélez and her team started doing this by reorganizing the structure of the ministry (Annex 1). The new organizational structure was based on functions and was meant to be supported by reliable information systems. To uplift morale and generate buy-in to this change, Minister Vélez focused on tangible, physical changes to the ministry as well. First, she turned a dated, bare-bones office environment with minimal technology into an open co-working space with more furniture and better use of space. Second, she instituted a “customer service system” [Sistema de Atención al Ciudadano – (SAC)] on the first floor of the ministry, which consisted of a one-stop shop for citizens to get help with accessing any Ministry services and provide feedback.
As the space changed physically, so did the culture of the Ministry. First, Minister Vélez recruited a strong technical team with significant expertise. She led by example to demonstrate the kind of work ethic she expected of her team. She was a strict leader who always came in at 7 a.m. and stayed in the office until the job of the day was done but she also wanted to show investment in her employees so she supported workforce training programs to improve capacity in digital literacy, results-based management, and other technical functions that could foster effectiveness and efficiency. Minister Vélez and her team were able to promote buy-in from all ministry employees through open and transparent communication and by creating channels and routines for direct communication with her. The first Monday of every month, she held a planning meeting with the most senior ministry officials: vice ministers, the secretary general, and ICFES1 and ICETEX2 directors. Every subsequent Monday of the month, she would open the meeting to first include directors from different areas for budgeting and planning; then to include deputy directors to follow up on project implementation; and finally the last Monday of each month would be an open conversation conference for all employees to share and discuss policy ideas.
Finally, Minister Vélez prioritized improved organization of data and use of information systems within the ministry. This started with better organizing archived information and ensuring systems were in place to appropriately store and use routinely collected data (Annex 2). It also included making sure this data was publicly available to ensure accountability to all stakeholders.
While many of these moves consolidated the efforts of previous administrations to modernize the sector, they also caused tension between the educators in the ministry who called for pedagogical accompaniment and felt that the focus on modernization was overlooking other critical areas in need of reform.
1 The ICFES underwent also an important change from being the “Colombian Institute for the Promotion of Higher Education” to becoming the Institute in charge of Assessing and Evaluating all levels of Colombia’s education.
2 Colombian Institute for Educational Loans and Technical Studies Abroad (Instituto Colombiano de Crédito Educativo y Estudios Técnicos en el Exterior, “ICETEX”).
Implementation: Collaboration, Data, & Communication as Tools for Success
When leading an institution such as the Ministry of Education one has to manage a number of different stakeholders both internally (e.g. ministry, Cabinet, President) and externally (e.g. local secretaries of education, teachers, unions, the business community, parents, students, etc.). Thus, a Minister’s scope of action to implement change is heavily impacted by her ability to dialogue and negotiate with different stakeholders and to convey well-tailored messages to address their varied concerns.
A key factor contributing to Minister Vélez’s success was her ability to coordinate and collaborate with the wide range of interests that surrounded the education sector. She was able to do this well because she ensured that she had access to timely data on which to support her decision making and communication. This evidence-based strategy allowed her to more effectively disprove misconceptions and provide accurate information where needed. In addition, and perhaps more importantly, it allowed her to acknowledge accurate faults identified by any of the stakeholders, so that she could also set a timeframe to respond to them and show indicators of progress.
Local Secretaries of Education
One of the most difficult challenges to overcome when working at the federal level was coordination with local entities. The decentralization process that Colombia was undergoing exacerbated some of these difficulties as local authorities had varying levels of capacity to deal with the new mandates for which they were now responsible. The Ministry of Education had to work closely with local authorities to make sure that education policies designed at the federal level could be implemented effectively. There were several mechanisms for this cooperation. The first one echoed the way in which the Ministry had achieved internal buy-in: communication. Every three months, summits were introduced and almost all the newly appointed education secretaries convened to discuss and learn about the changes that were being promoted at the Ministry. These summits also gave them the opportunity to share best practices from the federal level and across local levels, and to ask for the institutional help they needed in order to transform local capacity.
Even though the success with which the local authorities were able to implement the educational revolution was uneven (mainly because it also depended on the size and wealth of each of the departments and municipalities), there were incentives promoted by the ministry that supported a good degree of implementation. For instance, Law 715 not only changed the formula for the distribution of resources to the regions, but it also attached them to the number of students enrolled in each school. This was a fundamental transformation of the incentives and logic with which local authorities functioned; now they were forced to increase enrollment to get more resources. This policy of “money following the students”, plus a policy designed by Minister Vélez and her team to distribute additional resources to areas where the vulnerable populations were, helped promote the access in an unforeseen manner. It also created a new problem: “phantom students,” which gave the ministry additional incentives to create, promote and audit accurate information systems. To address this unintended consequence, the ministry had to confront the data systems it had with data from other governmental agencies and an auditing system implemented with the ICFES.
Higher Education Institutions
Legislation preceding Minister Vélez’s term had near autonomy of higher education institutions. This had led to a large increase in access to higher education (from 22% of the total students who graduated from high schools enrolling into tertiary education in 1992 to 46% in 2002) but was not accompanied by any oversight to ensure quality. To satisfy the need for more regulatory control and standardization, one component of Minister Vélez’s reorganization of the Ministry of Education was the introduction of the Vice Ministry for Higher Education.
This change was important because it elevated the importance of higher education to the vice-ministry level and institutionalized a state policy process into the creation of a National Accreditation Board composed of universities representatives. This allowed for important and constant dialogue coordinated by the Ministry between the presidents of private and public universities, professors, the business community, and student unions to co-create and define the standards and certifications that would govern them. Stakeholders felt heard in this process, and their feedback was documented in the ECAES3 series, where both positive, those who view it as an opportunity to add structure and to redesign their programs, and negative reviews, especially regarding fear of losing autonomy and more government incidence, from university presidents can be read. Universities were incentivized to participate in this change from a low regulatory environment to a strict, but voluntary, accreditation process because of the appeal and prestige associated with the government certification that would be granted to programs that were deemed to be high quality. The certification process sparked competition among public and private institutions, thereby creating a higher quality and better-regulated system in a short period of time.
3 Examen de Estado de la Calidad de la Educación Superior (State Exam for Higher Education Quality), which was later renamed SABER – PRO and is administered by the ICFES.
Colombian Educators Foundation (FECODE) Union
FECODE is Colombia’s largest teachers’ union and it has traditionally served not only to protect the labor rights of teachers in the country but also to contribute to education policy. Minister Vélez’s administration is still the only that can claim that during her eight years in office there was not a single general strike. Alongside a mutual understanding to place teachers’ wellbeing at the heart of policies that govern them, four main reasons contributed to such an atypical relationship between Vélez’s ministry and FECODE.
Firstly, as with other stakeholders, Minister Vélez ensured open and regular communication routines with FECODE with a clearly defined agenda centered on teachers’ wellbeing and working conditions. She instituted monthly meetings between herself, her senior ministry team, and the leaders of FECODE. In this meeting, she would share updates from the ministry on policy and implementation progress and listen to suggestions and complaints from the union. The Minister appointed her General Secretary to monitor the agreements that were reached in these meetings and to keep all parties updated on progress. This process allowed for constant advancement in the union’s efforts to protect teacher rights and was seen as a win for both sides.
Secondly, before taking office Minister Vélez negotiated with President Uribe that one of the requirements for her to become Minister was that the teacher payroll had to be up to date and disbursed on time. Since FECODE’s main goal is to ensure the labor security of its members, the fact that the Ministry was delivering salaries on schedule created a strong foundation for a fruitful and stable relationship.
Thirdly, Minister Vélez was in a politically fortunate situation. Her predecessors had recently passed laws instituting an admissions process to become a teacher and a merit-based teacher evaluation system. Despite regional resistance to some of these laws, Minister Vélez was legally mandated to implement them and she was able to communicate these constraints effectively to justify her actions. Building on this, while it was often customary for politicians to ally themselves with FECODE during elections and then remain indebted during their administrations, Minister Vélez and President Uribe were not constrained as such. Thus, they could always remain firm and maintain their independence when dealing with FECODE. However, this never translated into active opposition because Minister Vélez and her team understood that teachers’ wellbeing is a critical element of a successful education sector.
Business Community
The business community played a prominent role in the reform by serving as key allies throughout the process. Building on President Uribe’s initial promise to protect the Minister of Education protection during his term, the business community had created a key source of stability for Minister Vélez which gave her the opportunity to promote large scale changes. During her time in office, local chambers of commerce and regional companies provided significant donations which suggested that the government was working alongside the business community, something that was unusual in Colombia at the time. To the general population, this was perceived as an endorsement of the ministry from a serious enterprise.
To maintain this support, Minister Vélez arranged monthly meetings with some of Colombia’s most important industry leaders and “Empresarios por la Educación” [Businesspeople for Education]. These meetings provided a space for accountability and an opportunity to solicit advice regarding the professionalization of a sector badly in need of capacity development among its workforce. The advice from these meetings ultimately led to the ministry obtaining technical support from a firm that specialized in organizational change and helped reinforce the actions pursued by the ministry.
Media
As she demonstrated with all stakeholders, Minister Vélez’ ministry was one that was open for dialogue and the profound transformations made the education sector a newsworthy topic that the media was eager to cover. The ministry was willing to communicate with the media and used it as an avenue to showcase its progress since this was the first time that the Ministry of Education had quality, publicly available data. The increased accessibility of information about the education sector meant that public interest increased. The Ministry faced a more informed population which scrutinized their actions and ultimately, created a higher level of accountability in the public sphere.
Outcomes: Successes and Outstanding Challenges
As a result of the changes implemented in Colombia’s Education Reform, there were significant improvements in access, quality, and information systems as mentioned earlier. Below are some additional highlights achieved during this period:
Literacy: Between 2002 and 2008, 1,017,934 adults learned how to read and write.
Higher Education: The number of instructors increased by 32.6% between 2002 and 2008, and their professionalization can be measured thanks to an increase in instructors with graduate degrees of 46% and those with doctorate degrees grew 87.2% in the same period. Dropout was also considerably reduced from 16.5% in 2002 to 12.1% in 2008.
Infrastructure: To control and improve the education inventory funds were tied to the improvement and regularization of the infrastructure. As a result, between 2003 and 2008 1,760 educational institutions had projects approved, which meant an increase in project approval from only 7% in 2002 to 27.2% in 2008.
Private education: Thanks to efforts in certifying and assessing the private institutions, the number of schools that were labeled as Regulated Freedom (i.e. certified, accredited or high-performing schools) rose from 33% in 2006 to 42% in 2009, and those labeled as Controlled Operation (i.e. sanctioned or low-performing schools) decreased from 31% in 2006 to 20% in 2009
Teacher Training: For the first time in Colombia’s history, teachers were able to enter the workforce after passing an evaluation. Between 2002 and 2008, 49,727 teachers and teacher directors were hired through competition (16%) and 14,265 teachers and teacher directors took the promotion evaluation.
Despite the significant progress Minister Vélez was able to accomplish, certain challenges persist in the education sector. Firstly, even though the center of her quality strategy was to set standards and implement student evaluations, some actors claim that pedagogy has not changed at the classroom level and that memorization and rote learning is still a common pedagogical method at the school level. Even though some teacher training programs were implemented to improve instruction, limited federal and local resources prevented the distribution of textbooks to all schools, forcing learners to rely on public libraries. Such an example highlights the stark inequalities that remain between the private and public schools.
Another ongoing challenge is the proposed transformation of the teacher admission process. Even teachers who went through this process (i.e. passed an entrance exam and underwent one year of training) were not necessarily appropriately trained to teach. Teaching manuals were provided to all teachers but workshop training to supplement them did not occur. As such, the admissions process did not improve teaching quality and demand for teachers meant that schools were not able to be as selective as they would like in their hiring.
Lessons Learned: Recommendations for a Minister of Education
Colombia’s experience during the Educational Revolution helps to highlight the importance of a strong Minister of Education in creating a clear vision and taking decisive actions. The ambitious goals that were outlined since the presidential campaign thanks to dialogue with key stakeholders were constantly co-constructed at different levels. The public had access to this progress thanks to transparency in the education indicators and the promotion of public discussions.
Transformation of a sector cannot be a one-person job, so the importance of working alongside a strong team is vital for any leader’s success. In Minister Vélez’s case, she was able to summon a team of well-respected professionals in the education sector, who were themselves insiders with technical knowledge. Their competence was found not only in the highest offices, but also at middle management levels to lead each of the workstreams. The leaders of Colombia’s educational policy today emanated from this time. Perhaps, the inclusion of more geographically diverse team could have helped to point out solutions to some of the problems the implementation encountered.
Another important factor was that as a coordinating agent of the educational sector, Minister Vélez invited local authorities to assess the policies and their implementation. Their presence and participation helped tailored the national policies to local realities that they knew from first-hand experience. This two-way communication was possible because of the ability to listen, learn, and act with humility when people perceived certain actions as mistakes. The fact that Minister Vélez was also willing to walk alongside her teams in the territories also created a sense of proximity that allowed her to put a face to the stories she was telling with precise data and accurate information systems. She was able to steer the public conversation away from general strikes and into more constructive nuances, which created a better-informed society that held the ministry, local authorities, and school staff accountable. The alliances formed with civil society, the media, and the business community were also a central factor for the buy-in the Educational Revolution had from the public.
Her ability to align herself with the agenda of the President, and to count on his support, gave Minister Vélez the stability that was needed in the sector to stay on as minister for eight years, making her the second longest-lasting minister in the recent history of Latin America. Education policy is a long-term project, so being able to think and implement policies throughout two administrations allowed the sector to understand and cope with the changes gradually, but most importantly, to see the results of each of the actions that were being put into place.
Another fundamental lesson was that, thanks to her prior knowledge of the sector acquired while serving as Secretary of Education in Bogota, she was able to think about the sector comprehensively. This also allowed her to come up with a National Strategic Plan that shaped the guidelines and goals of her administration since the very first days. Instead of promoting incremental changes in small areas, she pursued an ambitious transformation of the sector as a whole.
The above was only possible because of the information systems that were installed. Up to date information was able to be conveyed from the territories to the ministry and back to detect problems and to act upon them. The coordination mechanisms that supervised and audited the information served to decide on agreements and to fix short- and long-term measurable goals that were monitored by dash-boards. This allowed for a periodic assessment of progress that disentangled the complexities of tackling the system as a whole.
At the time, two issues in Colombia had been spared from the ideological struggles between the left and the right: urban policy and education. Both were areas where a consensus was possible and where “soft reformism” was given fertile ground to promote better services for the overall population resembling an effective social democracy. Although many of the actions performed by Minister Vélez and her team were well known around the world, the way in which she implemented them made a big difference in the outcomes when compared to other cases in the region. Her example shows that with an understanding the importance of the human factor combined with data-based decisions, real change is possible, even in a context as challenging as the education systems in Latin America.
Bolman, L. G., & Deal, T. (1997). Reframing Organizations, Artistry, Choice, and Leadership, 6th Edition, San Francisco: Jossey-Bass Publishers, Inc.
Davis, I. (2010). “Letter to a newly appointed CEO,” in McKinsey Quarterly, McKinsey Company.
Deal, T. (1985), “Cultural Change: Opportunity, Silent Killer; or Metamorphosis?” in R. Kilmann, M. Saxton, R. Serpa, Gaining Control of the Corporate Culture, San Francisco: Jossey- Bass. pp. 292-331.
Delors, J. (1998). Learning: The treasure within. Unesco.
Reimers, F. (2019). Cartas para un Ministro de Educación. Cambridge.
Hauser, C. B. (2015). A Communication Strategy for the First Six Months in “Opportunity Knocking.”, Council for Advancement and Support of Education
Hackman, J. R. (1998) “Why Teams Don’t Work,” Leader to Leader, Winter. P. 24-31.
Kingdon, J. W., & Thurber, J. A. (1984). Agendas, alternatives, and public policies (Vol. 45, pp. 165-169). Boston: Little, Brown.
Kline, H. F. (1999). State building and conflict resolution in Colombia, 1986-1994. University Alabama Press.
McLaughlin, J. (1993) “Leadership Transitions: A Wide-Angle Lens,” in Harvard Institutes for Higher Education. Cambridge, MA: Harvard Graduate School of Education, vol. 2, no. 2.
Ministry of Education (MinEducación) of Colombia. (2010) “Colombian Educational Revolution 2002-2010. Action and lessons”. Ministerio de Educación de Colombia 2010.
Mintzberg, Henry, and Frances Westley. (1992). “Cycles of organizational change.” Strategic management journal 13, no. S2: 39-59.
Orlando Melo, J. (2017). Historia mínima de Colombia. El Colegio de Mexico AC.
Vélez, C. (2019). Building Institutional Capacity for Large Scale Educational Reform [ppt Slides]. Shared from lecture on March 2019 at the Harvard Graduate School of Education.
Annex 1: Re-Engineering of the Ministry
Source: Vélez, C. (2019). Building Institutional Capacity for Large Scale Educational Reform [ppt Slides]. Shared from lecture on March 2019 at the Harvard Graduate School of Education.
Annex 2: Information Systems
Source: Vélez, C. (2019). Building Institutional Capacity for Large Scale Educational Reform [ppt Slides]. Shared from lecture on March 2019 at the Harvard Graduate School of Education.
Methodology: Interviews
The interviews were conducted in person or virtually and consisted of 20-minute to two-hour in-depth conversations about the role and perceptions of these stakeholders who played a central role in Colombia’s Education Reform.
Persona
Cargo 2002 – 2010
1 Alberto Espinosa
Founder and member of Business People for Education
2 Angela Constanza Jerez Trujillo
Communications Coordinator of the Alliance, Education Commitment of All
3 Anibal Gaviria
Former Antioquía Governor
4 Cecilia María Vélez White
Former Minister of Education of Colombia, Former Secretary of Education of Bogota
5 Daniel Bogoya
Former ICFES Director
6 Fabio Sánchez
Professor Los Andes University (School of Economics)
7 Felipe Barrera Osorio
Professor HGSE & World Bank
8 Gabriel Burgos Mantilla
Viceminister of Higher Education
9 Himelda Martinez
Viceminister of K – 12
10 Isabel Segovia
Viceminister of K – 12 // Former Vice-president Candidate
11 Javier Botero Álvarez
Viceminister of Higher Education
12 Jorge Enrique Giraldo
Founder and member of Business People for Education
13 Jorge Orlando Melo
Historian and editor of the “Memorias de la Revolución Educativa” [Memories of the Educational Revolution]
14 Juan Pabo Caicedo
Chief of Staff of the Minister of the Interior – HKS
15 Juana Inés Díaz Tafur
Viceminister of K – 12
16 Margarita Peña Borrero
Former ICFES Director
17 María Figueroa
Seating ICFES Director
18 Maria Juliana Rojas
Specialist in K-12 at HGSE
19 Nohemy Arias
Secretary General of the Ministry of Education
20 Pablo Correa
El Espectador / Journalist and analyst
21 Pablo Navas
President of Los Andes University
22 Roxana Segovia de Cabrales
Secretary of Education of Cartagena y Viceminister of K – 12
In October 2016, Brazil’s Minister of Social and Agrarian Development, 1 Osmar Terra, introduced a collaborative early childhood development intervention called the Criança Feliz Program (PCF). In the preceding 11 years, Brazil had reduced poverty from 22.4% in 2004 to 8.7% in 2015 and extreme poverty from 7.6% in 2004 to 2.4% in 2015 thanks to the conditional cash transfer program Bolsa Familia (Annex 1). However, even though research had found that children from families benefitting from Bolsa Familia had a cognitive development 65% above average, cash transfers were not enough to break the poverty cycle and overcome the challenges of violence in the country in the long run. With 15 million children under the age of four and high rates of poverty (Annex 1 & 2), there was a great need for a transformational intervention like PCF which involved regular home visitations as the basis for multisectoral early childhood development support. Now operating at full scale after just two years, PCF has made it possible for nearly 500,000 children and 85,000 pregnant women in Brazil to receive home visits every week, a total of almost 2.4 million visits a month in over 2,000 municipalities.
To implement such an instrumental program in such a short period of time, Terra relied on his ‘educational’ political style. He believed that by explaining the evidence underlying policymaking to people, he could gain their support for his cause. However, he knew that this would take time and so he began laying the groundwork for what would become PCF more than a decade prior, in 2000.
Using Evidence to Create Opportunity
The year 2000 was a turning point for research on early childhood development. James J. Heckman won the Nobel Prize of Economics for his work demonstrating long-term returns on investment in early childhood programs for children under five and Carlsson, Greengard, and Kandel won the Nobel Prize of Medicine for their research on the critical neural connections and learning formed during early childhood. These new advances laid an evidence-based foundation for investment in stimulation, quality care, and security of children to support their emotional and cognitive development, and ultimately their education and economic attainment as adults.
At this time, Osmar Terra was the coordinator of the social development program Comunidade Solidária under President Cardoso. There was a clear opportunity for Brazil to take note of this research, as local studies had shown that child-recipients of social aid were 35% less cognitively developed than the average Brazilian child and only 8% of poor families in Brazil had any books in their homes. In response, he seized the opportunity to create the Committee on Integral Development of Early Childhood (CODIPI), where he brought together actors from civil society and across government to educate every single relevant stakeholder on the importance of early childhood interventions. The process for building a movement for early childhood in Brazil (that would eventually lead to PCF) had begun.
1 This ministry was combined with the Ministry of Sports and the Ministry of Culture to form the new Ministry of Citizenship in January 2019 that continues to manage PCF and is led by Minister Terra.
Prioritizing a Common Goal Together
By 2002, Terra had not succeeded in building as much support for his ideas as he had hoped and due to a change in government, the CODIPI was dissolved. Nevertheless, Terra kept his vision in the back of his mind, and when he became Secretary of Health of Rio Grande do Sul state in 2003, he knew it would be his priority. In April 2003, Terra launched a new version of the CODIPI for his state, which included 17 large civil society organizations and representatives from the Secretariats of Culture, Education, Health, Work, Citizenship, and Social Assistance. He knew that intersectoral collaboration was key to his effort and bringing different actors on board from the beginning, particularly his secretarial counterparts, would be critical to his success.
With the help of the new CODIPI, Terra launched the Primeira Infancia Melhor (PIM) program, the first home visitation program in Brazil (Annex 3). Intersectoral and inter-ministerial collaboration was at the center of this initiative since any home visit could yield a variety of challenges. If, during a home visit, a child was found with a medical condition, the Secretariat of Health had to intervene. If a child had a learning disability, the Secretariat of Education had to get involved. If the family belonged to a particular ethnic group, the Secretariat of Culture would ensure that the home visitor had culturally relevant activities for the child. If a family struggled with employment, then the Secretariat of Work needed to act. The underlying idea was that the government would not act in siloes, but rather work in a deeply coordinated way, since any child in an underprivileged environment would need the concerted efforts of different parts of government to achieve his or her full potential.
The spirit of collaboration was also present in the partnership that Terra started with Celep. They were the center responsible for implementing Educa a tu Hijo, the Cuban program that had inspired PIM. This partnership provided both technical support and legitimacy to the undertaking of PIM.
Institutionalizing Collaborative Efforts
To date, PIM has survived governments from four different political parties and continues to serve around 65,000 children every week. Building on such a successful in-country intervention was critical to further expand support and collaboration for early childhood development interventions across Brazil. In 2006, national legislators passed the State Policy for the Promotion and Development of Early Childhood (Ley Estatal no. 12.544) and in 2007, thanks to the leadership efforts of the Bernard van Leer Foundation, the National Network for Early Childhood (RNPI) was created. It brought together a number of civil society organizations, government agencies, private sector entities, and others. It was a massive coalition with far-reaching technical and political power all across the country. The coalition demonstrated this power in 2010 when it managed to pass the National Plan for Early Childhood (PNPI) at the National Council for the Rights of the Child and Adolescent (Conanda).
The institutionalization of RNPI created conditions that would later allow for PCF to be successful.
Thus, in 2011, with early childhood already as a national priority, Terra began setting the ground for PCF. In May 2011, he created the Parliamentary Front for Early Childhood, a cross-party group with over 2000 deputies. The Parliamentary Front’s main goal was to achieve a Legal Framework for Early Childhood that would guarantee the rights of children in different public policy sectors, aiming to promote the integral development of the child. This would ensure that every municipality and every state would have an action plan, a budget, rules, and laws to guarantee the rights of children. With this goal in mind, the Parliamentary Front organized the 1st International Seminar: Legal Framework for Early Childhood in April 2013 to spread awareness and spark conversation across society. By December of that year, they were able to pass the Legal Project for Early Childhood (Projeto de Lei 6.998/2013). In the words of Minister Terra, “Everybody’s mandate is limited, but policies should be passed to stay.”
Using Evidence and Communication to Galvanize Support
Concurrently, Terra was working on developing an executive leadership course on early childhood development in partnership with the Maria Cecília Souto Vidigal Foundation, the INSPER business school and the University of Saõ Paulo, to be held at the Center for the Developing Child at Harvard University. His idea was that if politicians and senior technicians from the administration learned about early childhood from world experts, they would come back to Brazil as serious advocates. In most cases, the course was free of charge for Brazilian politicians and therefore few renounced the opportunity to receive training from Harvard.
Participants were required to stay at Harvard for a week during which time they designed a project that they were meant to present to Parliament and implement upon their return to Brazil. This single initiative proved to be incredibly effective. In the words of the spokesperson of the Parliamentary Front, “Everybody changed at Harvard.” Over the course of a few years, around 400 Brazilian politicians and bureaucrats went to Harvard and came back as champions for early childhood development.
In the following years, the RNPI, the Parliamentary Front, and a growing number of administrators and politicians advocated for early childhood programming – organizing a second international seminar with broad participation from civil society, four regional seminars and two interactive public audiences, among other initiatives. At the same time, there was a media campaign that was staged in partnership with national television channels to raise awareness about the importance of early childhood care. For instance, the Maria Cecília Souto Vidigal Foundation sponsored a documentary, O Começo da Vida (The Beginning of Life), which was screened in cinemas across 21 Brazilian cities in 2016 to more than 21,000 viewers. Bem Estar, a popular daytime television show, decided to increase parental awareness by dedicating five minutes of their show to early childhood education.
With such broad support and building on the ongoing success of PIM, the Legal Framework for Early Childhood was finally passed through the Federal Law no 13.257/16. Five years after creating the Parliamentary Front, and three years after launching the Legal Project for Early Childhood (Projeto de Lei 6.998/2013), the rights of the child were now hard law thanks to this Legal Framework. PCF began in October 2016 as a direct consequence of this Federal Law.
2 This program continues to this day with approximately 50 politicians participating every year.
Collaborating for Implementation across Government
Minister Terra knew that enacting a policy was just the beginning, implementation was the real test. He also knew that for PCF to really have an impact, he needed the involvement of different parts of government and different sectors of society (Annex 4). The Ministry of Social and Agrarian Development (now Ministry of Citizenship) would coordinate the efforts through the Secretariat for the Promotion of Human Development. However, to be implemented collaboratively, PCF needed a shared management structure. As such, a number of ad-hoc management committees were created at the national, state and municipal levels.
The National Management Committee housed representatives from the Ministries of Education, Health, Human Rights, Culture and Social Development in what they called the ‘interministerial government space.’ This space was a place where everyone was on board with the mission of implementing PCF and thus it served as a place to coordinate and solve technical issues, rather than arguing about objectives. This intersectoral committee was created by presidential decree, giving it the formality and gravitas to ensure that each ministry would take it seriously. The management committee had high-level representation from each ministry, and it was therefore a place for decision-making, rather than day-to-day collaboration. To get things done, they created the Technical Group, under which a number of inter-ministerial working groups would coordinate efforts.
An example of collaboration that has been achieved by the Technical Group and the National Management Committee is the redesign of the notebook that mothers receive when they have children. Traditionally, the Ministry of Health would give a notebook to the mother with child health tips. Now, since the creation of the National Management Committee, these notebooks include information about child development milestones and cultural specificities contributed by other ministries. Other examples of collaboration include a guide for visitors for children with disabilities and the development of training materials and workshops for both visitors and families.
Overall, the key roles of the National Management Committee are to strengthen the intersectionality of the program, to approve training and program resources, to make decisions about the stages of the program, and to agree on regulatory instruments that distribute responsibilities for different policies. One of its main responsibilities is to set the intersectoral budget. As coordinator of the program, the Ministry of Citizenship decides the home-visiting budget, which it distributes to the municipalities through the National Fund of Social Assistance. They decided to use this fund so that the funds would flow directly from the ministry to each municipality, avoiding intermediaries and countless individual contracts.
However, a budget for home-visiting is not enough to ensure the success of PCF. It is important that each ministry allocates funds to collaborate on the intersectoral needs that emerge from the visits. The National Management Committee is the place where the ministries negotiate the allocations that each ministry will contribute to PCF.
At the state level, similar Management Committees exist but are composed of representatives from State Secretariats. The role of States is to monitor the implementation and to give technical assistance to the municipalities. To achieve this goal, States hire multiplicadores (there are 89 across the country). They are professionals who are trained by National trainers, who in turn go on to train local coordinators, who train the local visitors. This modality of waterfall training has led to a number of implementation problems; however, it was the only way that Brazil could scale the program to over 2000 municipalities in just one and a half years.
At the municipal level, Municipal Management Committees are much more operational in scope. They discuss, support, and approve operational issues of the program. For instance, they identify the beneficiaries of home visits, hire and organize local training for visitors, follow up with different sectoral responses on the demands that they identify, and coordinate with local NGO networks. At the municipal level, intersectoral collaboration is often informal and they escalate any challenges to the state level.
A final component of Brazil’s interministerial implementation effort is its integrated information system, Cadastro Único, which allows different ministries to identify families and work from the same data. This has been an important tool because without it the registries of potential beneficiaries housed by each ministry varied, thereby leading to coordination problems and leaving people unattended. This has also allowed for more effective monitoring and evaluation of implementation across ministries.
Ongoing Challenges
No program is perfect and despite the strong inter-ministerial implementation structure in place, PCF continues to face some challenges. At the municipal level, some committees are more effective than others at implementation. One of the reasons for this is insufficient preparation. Brazil’s waterfall method of training managed by each State has created some disconnect between the original ideas and the actual practice, resulting in resistance from some municipalities. In one case, Terra’s involvement of civil society meant that NGOs like the Pitagoras Foundation were willing to collaborate with municipalities to support implementation. Another idea to bridge the informational gap between those at the core of PCF and each municipality is to develop an online education system that educates on the evidence base behind PCF and effectively communicates the different roles of actors across sectors and levels to allow for more effective and collaborative implementation.
Similarly, PCF has encountered some resistance from families themselves who thought they would lose their Bolsa Familia cash transfer or they suspected control from the Conselho Tutelar, an organizational structure that looks after the rights of children. Given the size and scale of Brazil’s 5,575 municipalities, this is likely to be an ongoing challenge, but it makes clear that communication is a critical component of successful implementation and that effective communication strategies must continue alongside implementation.
Conclusion
The successful implementation of PCF has been the consequence of a long-term undertaking. The ingredients for success were the following: a passionate, knowledgeable and energetic leader; a robust body of scientific evidence that backed the intervention; a number of successful in-country local home-visiting programs;3 a broad civil society coalition organized as a formal network; a parliamentary coalition with representatives from all political groups; constant efforts to align society under the flag of early childhood advocacy; and the articulation of shared management structures.
Minister Terra used a number of methods to create buy-in for his ideas such as organizing seminars and public audiences, developing courses, and creating audiovisual materials. The allies that he gained by opening up decision-making structures to stakeholders, as in the case of CODIPI, allowed him to achieve the necessary milestones that he needed, such as a legal framework, to implement PCF successfully.
Today, after almost three years, PCF has survived a change of president in Brazil and it grows day by day as more and more municipalities voluntarily sign up for the program (Annex 5). PCF has demonstrated the power of ideas and collaboration and as Brazil as a whole, both within and outside of government, grows more accustomed to debating ideas, building coalitions, and acting together, it is expected that more and more, different parts of government, NGOs, and the private sector will work together towards solving Brazil’s greatest challenges.
3 Although this case only mentioned PIM, several other state and local programs were implemented after PIM.
Harasawa, E., Pereira Grangeiro, G., et al. (2018). Manual do Pesquisador. Ministério do Desenvolvimento Social.
Harvard Kennedy School Multimedia Case on Criança Feliz.
Interview with Ely Harasawa, head of the Secretariat for the Promotion of Human Development in Brazil (2019).
Interview with Gilvani Pereira Grangeiro, director at the Secretariat for the Promotion of Human Development in Brazil (2019).
Ministério do Desenvolvimento Social e Agrario. (2017). Programa Criança Feliz, A intersetorialidade na visita familiar.
Secretaria de Avaliação e Gestão da Informação. (2019). Avaliação de implementação do programa criança feliz relatório final. Ministério da Cidadania.
Terra, O. (2016). Avanços do marco legal da primeira infancia. Frente Parlamentar Mista da Primeira Infância. Câmara do Deputados. Centro de Estudos e Debates Estratégicos.
Verch, K. (2017). Primeira Infância Melhor: Transforming the Attention towards the First Years of Life in Latin America: Challenges and Achievements of a Public Policy in Southern Brazil. Banco Interamericano de Desarrollo.
“If the agricultural sector does not invest enough, the cases end up in the hospital and the burden goes to the health sector to treat malnutrition”
Dr. Kesetebirhan Admasu served as Minister of Health of Ethiopia from 2012 to 2016. Upon entering office, Ethiopia had been making progress toward reducing stunting from 67% in 1992 to 44% in 2011, but significant rural-urban and regional variations meant that malnutrition persisted as one of the leading causes of infant and child mortality.
The Government of Ethiopia had already begun on a path towards heavy investment in nutrition including the reduction in stunting, wasting, anemia, and dietary diversity outcomes, beginning with the establishment of the National Nutrition Program I (NNP I, 2008-2015). Further recognizing the importance of nutrition as a pillar for human capital development and economic growth, Minister Admasu, along with Deputy Prime Minister, H.E. Demeke Mekonnen, launched the Seqota Declaration in July 2015, a high-level commitment by the Ethiopian government to end stunting in children under two years by 2030. Minister Admasu knew that incorporating nutrition goals and actions into existing programs across sectors could enhance their nutrition sensitivity and thus their likelihood of improving nutrition outcomes. Thus, the Declaration was accompanied by the launch of the National Nutrition Program II (NNP II, 2016-2020) and the National Nutrition-Sensitive Agriculture Strategy (2016-2020).
The causes and consequences of suboptimal nutrition span many sectors (such as agriculture and health) and thus the improvement of nutrition outcomes necessitates multisectoral coordination. Despite their expressed interest, policymakers struggle to create sustainable multisector policies and continue to address these issues in a siloed fashion, missing the opportunity to create even greater outcomes from the integration of these spheres. This case study will examine the Seqota Declaration to show how Ethiopia has made nutrition a national and inter-ministerial political priority, enabled consensus-building across sectors, and established coordinating bodies at the national and regional levels to implement.
NNP I: Preliminary Efforts towards Intersectoral Collaboration
Agriculture, health, and nutrition are mutually reinforcing sectors. Agriculture constitutes 40% of Ethiopia’s GDP and 80% of exports, and 75% of Ethiopians’ livelihoods depend on rain-fed agriculture. While agriculture and health are often administered as disparate entities, nutrition serves as the link between these two, with dietary intake closing the value chain from agricultural productivity to improved health outcomes. As part of this more multisectoral approach, the sector has shifted from purely nutrition-specific interventions, such as exclusive breastfeeding and optimal complementary feeding, to include nutrition-sensitive interventions, such as water, sanitation, and hygiene, and food fortification.
The NNP I that Minister Admasu inherited was focused on “immediate causes of suboptimal growth and development” and the effects of nutrition programs on malnutrition. In particular, there was a focus on integration and coordination across nutrition-specific interventions that were supported by “evidence-enhanced decision making.” Nutrition programs were scaled up and an implementation platform was created in the form of the National Nutrition Coordinating Body (NNCB) and the National Nutrition Technical Committee (NNTC).
The NNCB involves 13 government sectors and is primarily led by the Minister of Health, with the Ministers of Agriculture and Education as co-chairs. It meets every six months and develops an annual work plan to ensure that various sectors are mainstreaming nutrition activities into detailed sector-specific plans, allocating budget to nutrition interventions, and assigning focal persons to work on nutrition. The NNTC, which also involves 13 government sectors and nongovernmental stakeholders, has three steering committees on program management, food fortification, and monitoring and evaluation. In addition to the NNCB, the Ethiopian government established Regional Nutrition Coordinating Bodies (RNCB) in most regions, as well as coordinating bodies at the woreda level.
Nutrition interventions under NNP I were intended to cut across sectors through the “Nutrition-Sensitive Agriculture Strategy, National Food Security Strategy, National Health Sector Transformation Plan, National Food Fortification, and the National School Health and Nutrition Strategy.” This multisectoral coordination was able to demonstrate some improvement in outcomes but was not fully effective in creating the intended outcomes.
The Seqota Declaration: Interministerial Support for Transformational Change
Improving nutrition to achieve sustainable development was the core vision of the Ethiopian government. However, it could not be done using traditional methods and did not pertain to only one sector. There was a need to tackle the issue from several angles by engaging different sectors in order to deliver high impact nutrition-specific, nutrition-sensitive, and infrastructure-smart interventions. Thus, the Seqota Declaration was unveiled by the Ethiopian government, led by Minister Admasu, in July 2015 to end stunting in children under two years by 2030. The Seqota Declaration builds on and supports the implementation of NNP II which highlights the “Five Building Blocks of Effective Nutrition Governance” as consensus building and coordination, political commitment, financing, service delivery capacity, and transparency and accountability.
Due to its ambitious nature, the Seqota Declaration Implementation Plan is divided into three distinct phases (Figure 1) to be executed over a 15-year period. Although they each have different specific goals, they are all part of a bigger picture, which intends to promote and ensure a smooth transition/path to success. During the innovation phase (2016-2020), new and innovative ideas are being tested out in order to generate evidence for interventions, while the expansion phase (2021-2025) involves increasing the coverage of the lessons learned from the innovation phase to reach more vulnerable communities. Finally, the scale-up phase (2026-2030) will involve national scale-up throughout the country. The innovation phase is being implemented in 33 select woredas (districts) in Amhara and Tigray regions where stunting prevalence is high and over 4 million people are entirely dependent on rain-fed agriculture and animal husbandry.
Figure 1. The Three Phases of the Seqota Declaration
The Seqota Declaration has ten multisectoral strategic objectives as outlined below and is implemented by six federal sectors (Ministry of Health; Ministry of Agriculture; Ministry of Water, Irrigation and Energy; Minister of Labor and Social Affairs; Ministry of Education; Ministry of Women, Youth, and Children). In addition to these six ministries, development partners and community organizations are also involved.
Strategic Objectives of the Seqota Declaration
Improve the health and nutritional status of adolescents, women, and children.
Ensure 100% access to adequate food all year round.
Transform smallholder productivity and income.
Ensure zero post-harvest food loss.
Enhance innovation around the promotion of sustainable food systems (climate-smart).
Ensure universal access to water supply, sanitation, and adoption of good hygiene practices.
Improve the health and nutrition status of school children.
Improve the nutritional status of pregnant and lactating women and children through PSNP interventions.
Improve gender equity, women’s empowerment, and child protection.
Improve multi-sectoral coordination and capacity.
Interministerial Collaboration in Practice
The Seqota Declaration has only recently been implemented and is still in its preliminary innovation phase. Thus, it is not yet known if Ethiopia will reach its goal of reducing stunting among children under two by 2030. However, there is still much to be learned from its ambitious approach to harnessing the efforts of six different ministries to address one significant challenge. This section will highlight certain elements of inter-ministerial collaboration that have been put into practice in Ethiopia as part of its journey towards achieving the Seqota Declaration.
Demonstrating Political Leadership and Commitment
The bold ambition of the Seqota Declaration would never have occurred without strong political leadership and commitment. However, equally important was the consultative process that was used to inclusively develop the Declaration and create local ownership and buy-in. At the federal level, this commitment to making the Seqota Declaration a priority could be seen through the political capital spent by the Deputy Prime Minister to get the commitment of the two Regional Presidents of Amhara and Tigray. At the regional level, this leadership commitment could be seen through the financial investment made towards the Declaration, at an amount which was higher than that of the federal government. This latter shows the deep interest of the Regional Presidents for the successful implementation of the initiative in their respective regions.
Both governmental and non-governmental officials highlighted four salient drivers of this political prioritization and movement toward nutrition-related multisectoral collaboration:
The international community’s emphasis on reducing undernutrition, specifically the MDGs, SDGs, and increased donor funding towards these priorities.
The 2012 Cost of Hunger in Africa study which showed that 16.5% of Ethiopia’s GDP was lost to child undernutrition through healthcare costs, loss in education, and workforce absenteeism.
Field trips to learn from the experiences of other countries, particularly Brazil and Israel, at implementing inter-ministerial nutrition strategies.
Nutrition champions within Ethiopia like Minister Admasu, the Minister of Agriculture, and former first lady H.E. Roman Tesfaye.
For an initiative as ambitious as the Seqota Declaration, leadership commitment is key. The political leadership exhibited by the federal government through the consultative process at all levels facilitated local ownership of the Seqota Declaration. This latter has resulted in the Seqota Declaration becoming a higher priority for leaders at both the federal and regional levels. The meeting between the Deputy Prime Minister and African Development Bank president to mobilize more resources for the initiative.
Identifying Relevant Actors and Roles
Stakeholder mapping was a critical first step to effective collaboration both internally and with external government partners. It is impossible to mobilize and utilize all actors towards a common goal in a complementary fashion without knowing who they are and what they can do. Thus, the implementation of the Declaration began with a stakeholder mapping exercise to understand which actors were at play across various sectors. Figure 3 outlines the results of the stakeholder mapping exercises conducted in Tigray and Amhara.
Figure 3. Stakeholders Mapping in both regions (Tigray and Amhara).
Clearly Defining Collaboration in Context
Minister Admasu noted that in the past, “interventions in agriculture, health, and other sectors were not properly contextualized” and that everyone in government acted separately without keeping an eye on what was actually necessary to get the job done. To ensure that everyone actually knows what collaboration looked like, they adopted a clear collaboration framework known as the “Three Ones” which meant that there is “one goal, one plan, and one monitoring and evaluation system” in place for better coordination across sectors.
Key interventions that make up the overarching plan include:
Increase production and consumption of locally available, nutrient-dense crops.
Increase small-scale livestock ownership.
Expand irrigation potential to improve water-use efficiency and extend growing seasons.
Improve water supply quality and quantity in households, health facilities, and schools.
Improve access to hygienic sanitation facilities to address open defecation.
Improve delivery of direct nutrition interventions through the public health system.
These priority interventions were also supported by each sector’s individual response to nutrition, some examples of which are outlined in Table 1.
Table 1. Key Examples of Sectoral Contributions to Nutrition
Sector
Key Contribution to Nutrition
Ministry of Health
Strengthen and integrate nutrition-smart interventions (e.g., WaSH, environmental health, and health extension services) with other nutrition-specific interventions.
Ministry of Agriculture and Natural Resources
Pilot the establishment of 20 hectares modernized demonstration farms called Agricultural Innovation and Technology Centers.
Ministry of Livestock and Fisheries
Improve access to animal feed and support regulations that promote farmer productivity.
Ministry of Water, Irrigation, and Energy
Establish the Tekeze River Basin Authority to address the institutional vacuum for water resources planning and management.
Ministry of Education
Incorporate national school health and nutrition strategy in education programmes to better health and nutrition services for school-age children.
Ministry of Labor and Social Affairs; Ministry of Women, Youth, and Children
Improve the resilience of families in the Tezeke River Basin to economic shocks through the expansion of the Productive Safety Nets Program while improving the nutrition status of children as well as pregnant and lactating women.
Building on Existing Collaborative Efforts
It was critical to build on existing government structures to catalyze progress. At the national level, multi-sectoral coordination is ensured by the two national nutrition committees, known as the National Nutrition Coordination Body (NNCB) and National Nutrition Technical Committee (NNTC). These two national entities have different goals as the NNCB is responsible for providing policy and strategic decisions related to the NNP. However, the NNTC works under the NNCB, and is responsible for the technical work related to the federal level NNP coordination.
At the regional level, there is a similar structure, known as the RNCB and RNTC. Figure 4 shows the level of integration and coordination built into the organizational structure below both the NNCB and NNTC.
Figure 4. Inter-ministerial Coordination Structure for both the NNCB and NNTC
Institutionalizing Flexibility and Coordinating Mechanisms
Traditional methods of governance and coordination, such as the top-down approach, were insufficient for this ambitious initiative. In fact, in the past, there had been concerns about issues related to the bureaucracy of government, which limited intersectoral coordination mechanisms to exist only horizontally at federal and regional levels. Moving forward with the Seqota Declaration, establishing entities with people from different sectors that would be fully dedicated to the initiative was required.
Thus, the creation of Program Delivery Units (PDUs), three in total, are a tangible “embodiment of intersectoral government.” PDUs are small teams of multisectoral experts placed in the federal, Amhara, and Tigray President’s offices to secure higher-level political commitment to regional nutrition activities, to ensure accountability to the highest level of the regional government, and to provide technical leadership and performance management support.
Figure 5 shows the composition of a single PDU and demonstrates how it can operate horizontally across sectors as well as vertically through different levels of government to ultimately form a team with diverse nutrition expertise proximal to executive power.
Figure 5. Program Delivery Unit (PDU) Composition
Innovating to Support Collaboration
Minister Admasu once said that “intersectoral collaboration is rooted in innovation” and that innovation relies on “learning by doing.” To this end, high-level delegations that traveled abroad to learn from other country experiences were able to bring back home some of the innovative ideas they learned and adapt them to the Ethiopian context. They realized that everything they learned could be translated to all of the sectors involved in the Seqota Declaration. For example, using technology to effectively manage water (i.e. Tekeze River Basin) would not only improve food productivity all year round (i.e. related to MOANR), but also increase coverage of safe and adequate water supply to households as well as the adoption of good hygiene through implementation of WASH strategies (i.e. related to MOH, & MOE). Improving water techniques was integrated through Agriculture Innovation and Technology Centers (AITCs), which provided the MOANR and its agencies with a platform to serve as demonstration sites for innovation. Lessons learned from the AITCs were intended to benefit MOANR directly but also with the expectation that new agricultural technologies would increase productivity and thus produce economic gains.
Monitoring and Evaluating Collaboratively
The “Three Ones” collaborating framework dictates that all nutrition-related monitoring and evaluation activities should be assessed under one integrated and unified system. The different sectors involved in the Seqota Declaration each have a list of key performance indicators that they are responsible for. These indicators are cross-cutting across sectors where relevant. For example, WaSH key indicators showed that the MOH needed to do more in terms of promoting hygiene and sanitation practices along with the MOE for targeted interventions at school. Another example is the dietary diversity score which falls under the health sector but baseline data showed that the score could not be moved by greater health promotion. This suggested that the score’s progress was being limited by factors controlled by other sectors such as the availability of diverse foods, gender inequity, or sociocultural factors.
With regards to monitoring, routine service and administrative records collected through sectoral information systems are used to provide information for timely monitoring, supervisory visits, and review meetings. Currently, the FMOH and UNICEF are working together on a pilot Unified Nutrition Information System (UNISE), a performance management tool that allows all sectors and partners to upload their targets and results so as to generate scorecards at the federal, regional, zonal, and woreda levels. This unified system is extremely important for progress towards the Seqota Declaration as it facilitates robust and continuous nutrition data management and becomes useful when seeking further investment. Dr. Sisay Sinamo, Senior Program Manager of the Seqota Declaration based in the FMOH, noted that having access to clear management performance indicator data during review meetings has allowed them (sector administrators and development partners) to make informed decisions at all levels.
With regards to evaluation, the Ethiopian Public Health Institute (EPHI) and Ethiopian Institute of Agricultural Research are charged with conducting official evaluations and undertaking “periodic assessments, operational research, and surveys to help identify program strengths, weaknesses, and key challenges.” Regional PDUs support this effort through the recruitment of data collectors and overseeing local data collection. Furthermore, regular “performance reviews” are part of the routine. The Deputy Prime Minister chairs quarterly meetings to assess the performance of all implementing sectors and development partners. The PDUs meet quarterly to share outcomes amongst each other and with relevant political leaders. Regional Presidents chair biannual meetings with regional actors and kebele and woreda administrators lead monthly meetings to share their performance with zonal and regional representatives.
Ongoing Collaborative Challenges
Today, approximately two years into the implementation of NNP II and the Seqota Declaration, it is clear that the NNCB has played an important role in bringing together various ministries. However, ongoing challenges with accountability and ownership persist – there is a persistent perception that nutrition is primarily a Ministry of Health (MOH) issue and that a lack of accountability across Ministries is the primary barrier to successful multisectoral coordination.
Even as nutrition has grown in national importance and public awareness, Ministry staff feel that with no cross-ministry reporting structures, there has been a lack of ownership and clarity about responsibilities for nutrition outcomes.
A separate but related challenge is how to improve coordination at the regional level. While many interviewees at the national level spoke about the leadership of the NNCB in nutrition governance, the Regional Nutrition Coordination Bodies (RNCBs) were rarely discussed. The function of the RNCBs in different regions appears to be variable, with ongoing work needed to strengthen them as coordination platforms.
A key component of accountability is the clear delineation of roles and responsibilities for all stakeholders. However, this role-definition for each sector is a challenge in the setting of multisectoral collaboration for nutrition governance. Deciding where the work of one Ministry starts and ends, and how it interfaces with other Ministries at the national, regional and local levels is a dynamic process with implications for political interests, leadership, budgeting, and accountability.
Key Takeaways
While Ethiopia is a unique context and has very specific cultural considerations, there are a few salient points which may be derived from this case and applied to a broader context:
Making nutrition a national political priority is a key component of fostering multisectoral collaboration and improving nutritional outcomes. Though funds may be limited, political commitment and thoughtful programs can often attract donor organizations to contribute resources. Additionally, political pressure can help to drive budget decisions towards investment in nutrition.
Multisectoral collaboration has contributed to a reduction in undernutrition rates in Ethiopia, largely due to the shift from nutrition-specific to nutrition-sensitive strategies. This approach is preferred as it addresses all determinants of nutritional status, including social and economic determinants.
Accountability structures are vital to effective coordination, monitoring and evaluation in multisectoral nutrition governance. Multisectoral collaboration holds great capacity to improve population nutrition by simultaneously addressing multiple determinants of nutritional status. However, implementation and evaluation of coordinated efforts are difficult without accountability structures at the local, regional and national levels.
Overall, while challenges remain, collaboration from the initial development of the Seqota Declaration has allowed for more effective coordination across all sectors. Fighting a common “enemy” together is always more valuable and effective than doing it alone and without a clear agenda.
Ethiopia Demographic and Health Survey 2011. Central Statistical Agency, Addis Ababa & ICF International, Calverton, MD.
World Food Programme. (2013). The Cost of Hunger in Africa: Implications for the Growth and Transformation of Ethiopia. Retrieved from WFP Report
Copenhagen Consensus. (2014). Nutrition: What’s the smartest post-2015 target? Retrieved from Copenhagen Consensus
European Union External Action. (2016). Implementation Plan (2016-2030): Summary Programme Approach Document. Retrieved from EU External Action
Federal Democratic Republic of Ethiopia. (2018). The Seqota Declaration: Innovation Phase Investment Plan (2017-2020).
Ruel M., Alderman H., The Maternal and Child Nutrition Study Group. “Nutrition-sensitive interventions and programmes: how can they help to accelerate progress in improving maternal and child nutrition?” Lancet. 2013;382(9891):536–551.
USAID. (2018). Ethiopia: Nutrition Profile.
WFP. (2013). The Cost of Hunger in Africa – United Nations World Food Programme – Fighting Hunger Worldwide. Retrieved April 29, 2019, from WFP
Glandon, D., Meghani, A., Jessani, N., Qiu, M., & Bennett, S. (2018). Identifying health policy and systems research priorities on multisectoral collaboration for health in low-income and middle-income countries. BMJ Global Health, 3(Suppl 4), e000970. BMJ Global Health
U.S. Department of State. (2018, August 10). U.S. Relations with Ethiopia. Retrieved April 26, 2019, from U.S. Department of State website: U.S. Department of State
NNP. (2016). National Nutrition Program 2016 – 2020. Ministry of Health.
Investing in health improves health outcomes and arrests the vicious cycle of poverty and illness.
The relationship between health and the economy runs both ways, lasts throughout an individual’s lifetime, and is intergenerational.
In 2000-2011, improvements in health contributed to an estimated yearly growth in full income of 1-2% across low- and middle-income countries.
Five core mechanisms explain how health affects poverty and the economy:
Financial protection: Removing financial barriers to access enables the use of health services when needed, and helps at-risk households avert impoverishing expenditures and poverty.
Education: The prospect of longer, healthier lives induces people to invest more in their human capital, as they are better able to realize future long-term gains in employment and income.
Productivity: Productivity is enhanced through the contribution of better health to increased worker capacity, lower rates of absenteeism, and less workforce turnover.
Capital investments: Heightened longevity in lifespan and higher incomes mean people save more for retirement – boosting the economy-wide capital available for increased investments.
The demographic dividend: With the right conditions in place, changes in population age structure with a growing and educated workforce create the opportunity for economic growth.
Case studies of three countries show how different policies were used to strengthen health systems, expand healthcare access, improve health outcomes, reduce poverty, and achieve economic growth:
Ethiopia: Investments expanded primary health care facilities to enhance access to health services and improved financial protection by launching a community-based health insurance scheme.
Brazil: Universal health coverage was achieved through primary care and family health teams by decentralization, expansion of human resources for health, and health system strengthening combined with welfare programs to stimulate demand for health and education.
Turkey: The Health Transformation Program scaled up family medicine-centered primary health care, increased health expenditures, extended insurance coverage to the poor, and created a unified health insurance system with equal benefits to improve health outcomes, diminish impoverishing expenditures, and contribute to economic growth.
The success of reforms in these countries was enabled by sustained political leadership, effective use of fiscal space, a focus on universal health coverage and financial protection, an emphasis on primary health care, and the combination of supply- and demand-side interventions in the health system.
Though very successful, these countries face the rapidly growing burden of non-communicable diseases that will place demands on the government health budget. Judicious investments will be needed to develop strong health systems underpinned by comprehensive primary health care designed to manage chronic illness. Only then can the achievements in health outcomes, poverty alleviation, and economic growth be sustained.
Investing in Health for Economic Growth and Sustainable Development
Health is a catalyst and a critical ingredient for achieving economic, social, and environmental goals, including alleviating poverty and economic growth. Targeted investments can produce improvements in health outcomes, provide financial risk protection to citizens when they are ill, and produce substantial societal benefits beyond health to help achieve Sustainable Development Goals (SDGs). Conversely, ill health produces poverty and hinders economic growth, while poverty drives ill health in low-, middle-, and high-income countries alike (Deaton, 2016), creating a vicious cycle.
This report provides an overview of the evidence of the benefits of investing in health, including the mechanisms that link health, poverty alleviation, economic growth, and human development. Using case studies of Ethiopia, Turkey, and Brazil, the report presents real-world examples to illustrate how better health translates into improvements in human development. The report draws on the evidence and country cases to discuss implications for policy makers.
Evidence from Ethiopia, Turkey, and Brazil points to several important characteristics that enabled the simultaneous introduction of large-scale health and social sector reforms, including sustained political leadership, effective use of fiscal space created by economic growth, a transition towards universal health protection and coverage, an emphasis on primary health care, and a combination of supply- and demand-side interventions in the health system to expand simultaneously financial coverage and access to healthcare services.
Multidimensional Nature of Poverty
Poverty has a multidimensional character. While level of wealth or income is often used as measures of poverty, poor quality of life also characterizes poverty, including access to affordable, quality health care and education, food security, employment prospects, and the availability of water, electricity, and adequate transportation infrastructure. Inequality in health, education, and employment opportunities hinders human development.
The multidimensional poverty index (MPI) and the human development index (HDI) are designed to capture the multi-faceted nature of human development and enable comparison across countries. Health is at the core of both the MPI and HDI. The MPI provides a comprehensive picture of poverty by bringing together multiple dimensions of human development. It uses severe, overlapping deprivations in health, education, and living standards to assess individual-level poverty (Alkire, Conconi, and Seth, 2014). Individuals deprived in three or more of 10 indicators (including nutrition, child mortality, and school attendance) are considered ‘MPI poor’. The HDI also incorporates the multidimensional nature of poverty, using three core indicators: life expectancy at birth, mean years of schooling compared to expected years of schooling, and gross national income per capita.
Health and Macroeconomic Growth
Investing in health may ultimately impact macroeconomic growth and other important economic indicators (Floud et al., 2011). A rich, long-standing literature explores the relationship between health and the economy, with many economists contending that health fuels economic growth (Fogel, 1994; Gallup and Sachs, 2001; Sachs, 2001; Bloom, Canning, and Sevilla, 2004). Fundamentally, economists and other researchers agree that the relationship between health and the economy runs both ways and lasts throughout an individual’s lifetime and between generations (Deaton, 2003; Floud et al., 2011). Health status has shown to be a significant predictor of economic growth, with improvements in population health spurring increases in gross domestic product (GDP) above and beyond other drivers (WHO, 1999).
The magnitude of the effect of health on macroeconomic indicators is substantial. The Lancet Commission on Investing in Health estimated that across low- and middle-income countries, improvements in health contributed to yearly growth in full income by 1-2% per year from 2000 to 2011 (Jamison et al. 2013). In South Asia alone, the yearly value of mortality decline was equivalent to 2-9% of average growth in income per person – half as large as the value of the total increase in GDP. The effects were even larger in sub-Saharan Africa, where major improvements in health have been achieved since 2000. In high-income countries, such as the UK, improvements in nutritional status alone account for an estimated 20-30% of GDP growth between 1800 and 2000 (Fogel, 1994; Floud et al., 2011).
The Relationship Between Health, Poverty, and Economic Growth: Global Evidence
Mechanisms for Achieving Poverty Alleviation and Economic Growth Through Investing in Health
Investments in health drive economic growth and poverty alleviation in a dynamic manner and over a long time horizon. The five core mechanisms through which health affects poverty and the economy are:
Financial protection: Ensures access to health services while preventing impoverishing expenditures.
Education: Longer, healthier lives encourage greater investment in human capital.
Worker productivity: Better health leads to increased workforce capacity, reduced absenteeism, and lower turnover.
Capital investments: Higher life expectancy and incomes result in greater savings and economic investment.
The demographic dividend: Changes in population age structure, combined with an educated workforce, drive economic growth.
A model of the dynamics of health, poverty, and economic development
Figure 1. Source (Report Authors 2016)
Financial protection: Financial protection when receiving care for illness impacts economic growth and poverty in two key ways. First, removing financial barriers to healthcare improves access to health services, and ultimately, enhances health outcomes. There is considerable evidence of the negative effect of user fees on access to health services, especially for the poorest segments of the population (Newhouse 1993). Removing user fees has been shown to immediately improve access to basic health services, including curative and preventive services, helping those in need to access services when they need them (Lagarde and Palmer, 2008). Second, financial protection reduces impoverishment by minimizing catastrophic health expenditures, which push households into poverty by forcing them to use savings, contract loans, or sell livestock and personal goods to cover health costs (Wagstaff 2008). Each year, an estimated 100 million people fall below the poverty line because of catastrophic health expenditures (WHO, 2010). Rates of catastrophic spending for health are usually higher in countries with limited prepayment systems or limited resources (Xu et al., 2003; Siroka et al., 2015). Investments in health systems that improve health and provide financial protection (through universal health coverage for example) reduce the incidence of impoverishing expenditures, decreasing the number of new cases of poverty.
Education: The prospect of higher life expectancy induces people to invest more in their human capital, including education. Better health translates into better attendance at school and better cognitive functioning. The prospect of longer, healthier lives incentivizes people to commit to years of schooling up-front, as they are better able to realize future long-term gains in employment and income. (Reference)
Productivity: Productivity is enhanced through the increased capacity engendered by improved health (Strauss and Thomas 1998; Straus 1986). High disease burden leads to higher rates of absenteeism and high turnover in the workforce, eroding productivity. Poor health in childhood – and even during pregnancy – can have long-term impacts on productivity (Buckles, Buckles, and Hungerman, 2008; Bleakley, 2010). A healthy, educated workforce is better able to use capital investments efficiently, thereby increasing total factor productivity across sectors. Workers’ contributions – whether in manual and non-manual tasks – increase, as physical and mental capacity increases with improved health. (Ref)
Capital investments: Better health translates into higher capital investments in countries with suitable institutional and economic conditions. Heightened longevity in lifespan means people save more for retirement – savings that boost economy-wide capital available for increased investments to spur economic growth. As incomes rise with higher education and enhanced productivity, the savings rates increase (Bosworth, Bryan, and Burtless 2004). Better health means people expect to be able to reap returns in future periods, inducing them to allocate more income to capital investments. (Ref)
The demographic dividend: As health outcomes improve, mortality falls and fertility declines, life expectancy of populations increases, providing an opportunity to reap the benefits of the demographic dividend. Demographic transition provides an opportunity to yield substantial economic benefits (Bleakley, 2010b; Bloom, Canning, and Fink, 2014). As fertility holds steady while life expectancy rises, the number of dependents initially rises. However, as this group grows older, a bulge in the working-age population emerges, leading to better dependent-working person ratios that broadly benefit the economy.
Health and Poverty Alleviation
Poverty is a critical step in the pathway that links health with economic growth. The relationship between poverty, the social determinants, and health has been extensively studied and analyzed: the impoverished often live in poor conditions, without proper access to water, sanitation, food security, or decent housing. Conversely, improved health plays a role both at individual, household, and societal levels in reducing poverty, ultimately boosting economic growth. Investing in health systems can improve health outcomes and also break the vicious circle of poverty and poor health (Wagstaff, 1987; Sachs JD, 2008).
At the microeconomic level, several studies support the conclusions of macroeconomic studies on the mechanisms through which health affects both the economy and poverty reduction (Thomas et al., 2003; Miguel and Kremer, 2004; Almond, 2006; Bleakley, 2007; Almond, Edlund, and Palme, 2009; Field, Robles, and Torero, 2009; Bleakley 2010a; Cutler et al., 2010; Lucas, 2010; Kremer et al., 2011).
Health and Sustainable Development
In 2015, the United Nations member states adopted the Sustainable Development Goals (SDGs), the successor to the Millennium Development Goals. SDG 3 aims to “ensure healthy lives and promote well-being for all at all ages” and is underscored by several health targets, including for communicable and non-communicable diseases, maternal and infant mortality, and universal health coverage. While many of the SDGs focus on climate change and environmental degradation more broadly, health is a key link between these environmental factors and human development. Health investments put countries on the path to reaching several of the SDGs, as benefits of investing in health extend beyond health system performance, by affecting poverty reduction, economic growth, and human development.
Evidence from Ethiopia, Brazil, and Turkey
Simultaneous progress in health, poverty alleviation, and economic growth make Ethiopia, Brazil, and Turkey suitable case studies for illustrating the mechanisms linking health, economic growth, reduced poverty, and sustainable development (Tables 1 and 2).
Since 2000, average yearly GDP growth has been substantial in the three countries, reaching between 2006 and 2011 to 10.9% in Ethiopia, 3.4% in Brazil, and 4.25% in Turkey. From 2000 to 2011, average life expectancy at birth rose in the three countries, from 51.9 to 62.1 years in Ethiopia, 70 to 73.6 years in Brazil, and 70 to 74.5 years in Turkey. Health spending per capita also increased between 2000 and 2011, on average rising each year by 16.2% and 10.5% in Ethiopia and Turkey respectively, and 9.9% in Brazil. (Tables 1 and 2)
Table 1. Socioeconomic Data
Demographics
Ethiopia (2000)
Ethiopia (2014)
Brazil (2000)
Brazil (2014)
Turkey (2000)
Turkey (2014)
Total population (millions)
66.4
97
175.8
206.1
63.2
75.9
Life expectancy at birth
51.9
63.44 (2013)
70.0
74.12 (2013)
70.0
75.18 (2013)
Total fertility rate (births per woman)
6.53
4.52 (2013)
2.40
1.80 (2013)
2.45
2.04 (2013)
Age dependency ratio (% of working-age population)
98.37
83.57
53.21
45.1
58.01
50
Urban population (% total)
14.74
19
81.19
85.43
64.74
72.89
Epidemiology
Prevalence of HIV (% of population ages 15 to 49)
3.2
1.2
NA
NA
NA
NA
Incidence of tuberculosis (per 100,000 people)
421
207
61
44
37
18
Estimated malaria cases
8,900,000
3,800,000 (2013)
1,200,000
230,000 (2013)
12,000
<50 (2013)
Diabetes (% burden of disease)
0.40
0.73 (2013)
2.43
3.56 (2013)
2.39
4.15 (2013)
Hypertension (% burden of disease)
0.23
0.49
0.55
0.70
0.70
0.98
Probability of dying between ages 30-70 from cardiovascular disease, cancer, diabetes, or chronic respiratory disease
15
19 (2012)
25
19 (2012)
18
24 (2012)
Economic
GDP at market prices (US$)
$8,242
$55,612
$657,216
$2,346,076
$266,568
$798,429
Poverty headcount ratio ($1.90/day 2011 PPP, % of population)
36.31 (2004)
33.54 (2010)
13.62 (2001)
4.87 (2014)
2.12 (2002)
0.26 (2012)
Antiretroviral therapy coverage
0
50
–
–
–
–
Under-five mortality rate
145.1
61.8
32
16.2
39.6
17
Maternal mortality ratio (per 100,000)
897
378
66
46
79
14.3
Source: World Bank Open Data, 2016. All US$ current prices for years 2000 and 2013 unless otherwise stated. Available online: http://data.worldbank.org/
Asterisk * represents data from the World Health Organization’s Global Health Observatory data repository. Available online: http://www.who.int/gho/database/en/
Between 2000 and 2011, the share of out-of-pocket expenditures as a proportion of total health expenditures fell in Brazil by 8.1 percentage points and in Turkey by 12.6 percentage points. In Ethiopia, out-of-pocket expenditures remained relatively stable, with a small decrease of 0.5 percentage points from 2000 to 2011.
The three countries also achieved substantial improvements in reducing poverty levels. Poverty – measured as the proportion of the population living on less than $1.90 per day – declined by 26 percentage points in Ethiopia between 2000 and 2011. In Brazil and Turkey, the poverty headcount ratio fell 2.4 and 1.6 percentage points, respectively, between 2006 and 2011. (World Bank 2016; Tables 1 and 2)
Table 2. Socioeconomic Data
Ethiopia
Brazil
Turkey
Year
2000
2013
2000
2013
2000
2013
Financing
Health expenditure per capita (current US$)
$5.4
$24.5
$264.7
$1,084.6
$197.2
$607.7
Total Health Expenditure (% of GDP)
4.45
5.06
7.16
9.67
4.95
5.59
Government Health Expenditure (% total health expenditure)
54.6
60.96
40.3
48.19
62.93
77.41
Out-of-pocket health expenditure (% of total)
35.95
35.38
37.95
29.93
27.65
14.98
Coverage
(All social insurance)
–
–
30.10 (2006)
28.34 (2012)
29.4 (2004)
34.6 (2012)
External resources for health (% of total expenditure on health)
16
32.3
0.54
0.06
0.06
0.04
Service Delivery
Human resource density (physicians per 1000 population)
0.021
0.022 (2010)
1.15
1.89
1.3
1.711 (2011)
Human resource density (nurses and midwives per 100 population)
–
0.236 (2010)
3.84
7.6
2.93 (2006)
2.402 (2011)
Skilled-birth attendance (% of total)
5.6
23.1
96.45 (2001)
98.1 (2011)
–
95 (2009)
DPT coverage (% of children ages 12-23 months)
30
77
98
93
85
98
Source: World Bank Open Data, 2016. All US$ current prices for years 2000 and 2013 unless otherwise stated. Available online: http://data.worldbank.org/
All the three study countries were able to improve health outcomes very substantially and demonstrated between 1995 and 2013 (the latest data available) high performance in key population health outcomes relative to GDP per capita and health spending per capita, and in relation to comparator peer countries (Figures 2A and 2B).
Figure 2A. Data sources: World Development Indicators, WHO National Health Accounts 2016
a) Infant mortality rate and b) under-5 mortality rate relative to health spending and GDP per capita
Figure 2B. Data source: World Development Indicators, WHO National Health Accounts 2016
c) Maternal mortality ratio and d) life expectancy at birth relative to health spending and GDP per capita
Ethiopia, Brazil, and Turkey achieved these improved health outcomes in different ways. The various paths pursued to improve health in these three countries, achieve economic growth, and reduce poverty provide valuable insights on how progress can be made across a variety of contexts.
Ethiopia: Ethiopia invested considerably in the health system to expand population coverage of primary health care facilities and improve financial protection through the launch of a community-based health insurance scheme.
Brazil: In Brazil, expansion of universal health coverage was facilitated by decentralization of decision-making (with community participation) and provision of health services to municipalities with financial incentives to expand primary health care, substantial investment and prioritization of primary health care through the “Family Health Strategy”, and the expansion of human resources for health.
Turkey: In Turkey, a comprehensive approach was adopted to improve the health system through the Health Transformation Program (HTP), with increased total health expenditures, the creation of a unified general health insurance system, expansion of financial protection for the poorest population through a non-contributory health insurance scheme financed by budget contributions, scale up of family medicine-centred primary health care, as well as improved access to public and private hospitals.
Ethiopia Case Study
In the 1990s, Ethiopia faced deep-rooted challenges in its health system. Low per-capita health expenditures characterized the health financing landscape. Out-of-pocket spending was above the sub-Saharan Africa average, contributing to already high rates of poverty. Population coverage of health services was low. A persistent budget deficit in the health sector hampered effective functioning of the health system (Dibaba et al., 2014).
Recognizing the shortcomings in the health system, the Government of Ethiopia launched the Health Care Financing Strategy in 1998, followed by substantial reforms to improve the functioning of the health system and population health (Ethiopian Health Insurance Agency 2015). Reforms focused on:
Enhancing government investments in the health system: The Government of Ethiopia expanded its investments in the health sector considerably. The government more than doubled its health spending between 2000 and 2011 from $5.6 in 1999-2000 fiscal year to $7.1 in 2003-04, to $16.1 in 2007-08 and $20.8 in 2010-11 (The Ethiopian Federal Ministry of Health 2010), with government health spending growing from 2.4% to 3.7% of GDP (WHO 2016). In real terms, government health expenditure rose 38% over this period (The Ethiopian Federal Ministry of Health 2010).
Fee waiver system: A fee waiver system was instituted to protect the “poorest of the poor” against the financial barriers to accessing health care. Eligibility of citizens for the fee waiver system is determined through community participation, with beneficiaries issued a certificate entitling them to free healthcare services (USAID, 2011). A majority of health facilities in the regions where the scheme has been implemented have revised their fee schedules (Health System Financing Reform Project 2011). Exempted services that do not charge fees include, but are not limited to: family planning, delivery, pre- and postnatal care, TB, leprosy, expanded program on immunization, voluntary HIV counselling and testing, antiretroviral therapy, and services to prevent mother-to-child transmission of HIV (USAID, 2011). Over 2.2 million waiver beneficiaries have been enrolled in the program in eight regions (USAID, 2011). While there have been some implementation challenges across regions, where the fee waiver and exemption system was fully implemented in Amhara, poor households now have better access to health services (Health System Financing Reform Project, 2011).
Community-based insurance scheme: As part of the health financing reforms, in 2011 Ethiopia also introduced a community-based insurance (CBHI) scheme. Supported by the Federal Ministry of Health, USAID, and local and international NGOs, the scheme is designed for people working in the informal sector, representing 89% of the total population (Derseh et al., 2013).
The CBHI has been implemented in three states that have a total population of more than 60 million (National Population and Housing Census of Ethiopia, 2007). A year after implementation, 45.5% of target households had taken up the scheme and more than 40,000 households have been enrolled to date (USAID, 2011; Derseh et al., 2013). Similar to the fee waiver system, enrollment is decided collectively at the community level (as opposed to the household level). Each member pays 5 Ethiopian Bir (ETB) registration fee (around US$0.25) and an annual contribution of ETB 180 (almost US$10). The federal government provides funding for the schemes. Local and regional governments provide a subsidy for poor households unable to afford the contribution. The federal government also provides financial support to the health facilities that provide healthcare services to CBHI members.
In 2013, an assessment of the CBHI program showed that the scheme led to increased utilization and intensity of care. This, in turn, generated more financial resources for the facilities providing healthcare services for CBHI members to expand service provision. Risk of impoverishment due to OOP fell by one half for those enrolled in the CBHI scheme (Ethiopian Health Insurance Agency, 2015).
Health Outcomes, Macroeconomic Growth, and Human Development
By 2011, major changes in healthcare delivery were apparent. Ethiopia has expanded coverage of health services with an eighteen-fold increase in health posts and a seven-fold increase in the number of health centers (Ethiopian Federal Ministry of Health, 2011). Primary health care coverage increased from 51 percent in 2000 to 92 percent in 2011.
There has been substantial improvement in population health outcomes (Derseh et al., 2013). Average life expectancy at birth rose one year per year from 2000 to 2011, increasing from 52 years to 63 years (World Bank 2015). Child mortality dropped from 166 in 2000 to 88 by 2011. Maternal mortality declined from 871 to 676 per 100,000 live births. Prevalence of stunting dropped from 58% to 44% from 2000 to 2011.
Macroeconomic indicators have also been strong since 2000. Ethiopia has achieved yearly per capita growth rates of 8.3% in the last decade (World Bank, 2016), with substantial investments in infrastructure and market development, including expanded road networks and more integrated markets.
Poverty Reduction and Financial Protection
Ethiopia has made remarkable progress in reducing poverty. In 2000, 56% of the Ethiopian population was living under the $1.25 poverty line (World Bank, 2016). By 2011, this proportion had fallen to less than 30%, a rapid decline in the share of the population living in poverty.
As health has improved, school attendance has increased substantially in Ethiopia. The proportion of the population without education declined 20 percentage points from 2000 to 2011 (from 70% to 50%). The Net Attendance Rate for primary education rose from 30% to 62% over the same time period.
The contribution of health to improvements in quality of life is best captured through a decomposition of the declines in the multidimensional poverty index (MPI). Figure 3 presents how much deprivation in education, health, and living standards contributed to the MPI in Ethiopia in 2011 as compared to the cross-country average. Among those classified as poor by the MPI, health contributed 28% of deprivation, lower than the cross-country average (34%), but more than the contribution of deprivation in education (26%) in Ethiopia in 2011.
Percentage contribution of deprivations in education, health and living standards to overall poverty, 2011
Figure 3. Source (Alkire, Conconi, and Seth, 2014)
From 2000 to 2011, the MPI for Ethiopia declined by 10%: less than the fall in the poverty headcount (33%) – a divergence driven by slower progress on living standards in the MPI than is reflected in the poverty headcount. Figure 4 compares the contribution of living standards, education, and health to the decline. Health contributed 18%, almost double the contribution of living standards, but less than the impact of education.
Percentage improvement in proportion deprived in education, health and living standards (2000-2011)
Figure 4. Source (Alkire, Conconi, and Seth, 2014)
Employment, Retirement, and Workforce Productivity
The Government of Ethiopia instituted improvements in its health system as part of a concerted state effort to pursue a “developmental state” model, which placed poverty reduction at its core. In doing so, Ethiopia has effectively used Overseas Development Assistance (ODA) to rapidly achieve government goals.
Since 2000, public investment in health and education has been a central feature of Ethiopia’s development strategy, augmented by ODA (World Bank, 2015). These efforts have led to major improvements in health, education, economic growth, and human development.
Notwithstanding successes, Ethiopia faces three interlinked future challenges. The first relates to an effective transition to a health system funded predominantly from domestic sources by reducing dependence on ODA. Strong economic growth and prudent fiscal management should help this transition. The second is the rapid demographic and epidemiological transition that will bring NCDs that will have to be effectively managed while addressing the infectious disease burden. The third relates to continued investments to achieve UHC, which must be underpinned by strong primary care to ensure access to comprehensive health services designed to address simultaneously infectious diseases, maternal and child health, and the rising burden of NCDs to sustain the gains in health, economic growth, and human development.
Brazil Case Study
Creation of the Brazilian Unified Health System (Sistema Único de Saúde) was part of a social movement, which underpinned the population’s fight against the military dictatorship to secure democratization and citizens’ rights. The 1988 Constitution, shaped by a democratic struggle and the Movement for Sanitary Reform (Movimento de Reforma Sanitaria), established health ‘as a fundamental right and a responsibility of the State’, with provisions to create a unified national health system (Atun et al., 2015).
The Unified Health System was established to achieve universal health coverage – part of a series of post-dictatorship social sector reforms in Brazil – aimed at improving health outcomes, providing financial risk protection, alleviating poverty, and reducing socioeconomic inequalities (Atun et al., 2014). Social sector reforms combined demand-side interventions, such as conditional cash transfers, and multisectoral action aimed at alleviating poverty by targeting social determinants of health. Reforms also combined supply-side changes to strengthen the health system in order to improve access for citizens, especially the most disadvantaged populations (Atun, 2015; Monteiro de Andrade et al., 2015).
The Unified Health System aimed to address high levels of infant and child mortality (especially from vaccine-preventable diseases), infectious diseases such as dengue, HIV, and tuberculosis, the rising prevalence of cardiovascular disease, and high levels of violence. Primary health care was strengthened as the platform for introducing multisectoral interventions and enhancing access to immunization and prenatal care, primary health care services, emergency care, and essential pharmaceuticals (many of which were manufactured in Brazil) (Paim et al., 2011; Atun, 2015; Monteiro de Andrade, 2015).
Alongside the prioritization of primary health care, the major characteristics of Brazil’s health system reform were:
Social participation and advocacy
Decentralization across a geographically, environmentally, and socio-economically diverse country
Expansion of human resources for health
These changes led to substantial improvements in average life expectancy at birth, which rose from 67.7 and 63.0 years for women and men in 1990, to 78.4 years for women and 71.6 years for men respectively in 2013. Infant mortality fell from 58 per 1,000 live births in 1990 to 15 per 1,000 live births in 2015.
However, in spite of these achievements, inequities in income distribution, levels of poverty, violence, and regional variation in health outcomes persist (Atun et al., 2015). Compared with 1990, premature mortality due to diabetes, as measured by years of life lost (YLLs) in 2013, increased by 43%. Furthermore, years of life lived with disability (YLDs) as a result of diabetes increased by 123% in the same time period (IHME 2013). In addition, alcohol misuse, tobacco smoking, undernutrition, and obesity have subsequently risen (Paim et al., 2011; Atun et al., 2015). These trends are concerning and, without concerted action, have major implications for the economic growth of the country.
Socioeconomic Welfare and Human Development
Between 1991 and 2008, Brazil’s gross domestic product (GDP) almost doubled from $608 billion to $1 trillion (constant US$), and per capita gross national income rose from $3,887 to $5,048 (World Bank 2016). The economic growth enabled the Government of Brazil to introduce ambitious welfare reforms, with policies aimed at stimulating and accelerating prosperity.
In 2008, five years after its establishment, the “Bolsa Família” conditional cash transfer program distributed over US$7 billion to 10.5 million families. In 2014, this amount increased to US$11.2 billion, accounting for 0.5% of GDP and covering one in four Brazilians (Paes-Sousa, 2013). Bolsa Família was an important contributing factor to the reduction in poverty by 27.7% during the administration of President Lula da Silva (Brandao Junior and Aragao, 2007).
Brazil has systematically increased the legal minimum wage since 2000. In 2010, the Brazilian Social Security System distributed pensions, retirement benefits, health benefits, and welfare assistance to 28 million Brazilians each month, amounting in total to US$153 billion, equivalent to 6.9% of GDP that year. The Social Security System offers financial protection to workers and their families in times of crisis precipitated by illness, accident, and imprisonment, and during periods of pregnancy and old age.
In addition to the Unified System for Social Assistance (Sistema Único de Assistencia Social), the Federal government’s anti-poverty program “Brasil sem Miséria” (Brazil Without Extreme Poverty) provides integrated support for the country’s poorest families – in particular those residing in the north and northeast regions of Brazil. Launched in 2011, Brasil sem Miséria expands Bolsa Família with the aim of eradicating extreme poverty by targeting 15 million of the country’s most neglected persons (Paes-Sousa, 2013). The program provides support for welfare, nutrition, health, education, housing, alongside employment and income support in order to raise per capita household income, enhance access to public goods and services, and improve access to employment and economic opportunities.
Policies go beyond cash transfers, seeking to develop capacity and skills for Brazilians to contribute more fully and more productively to the labor market. Together, these and other social and health initiatives (see Appendix Table 1 and Table 2) simultaneously invest in health and development, in an effort to create socioeconomic conditions conducive for economic growth.
Health, Poverty Alleviation, and Financial Protection: Achievements and Challenges
Social protection programs and financial protection have contributed to consistent improvements in alleviating poverty and reducing inequalities in Brazil (Paes-Sousa, 2013). Compared with other countries in Latin America (Appendix Table 3), Brazil has achieved lower levels of catastrophic health expenditures (Knaul et al., 2011), although out-of-pocket expenditures approaching 30% of total health expenditures in 2013 are relatively high (World Bank, 2013).
However, despite poverty alleviation and improvements in coverage of health services that are free at the point of delivery in the Unified Health System, some citizens incur catastrophic health expenditures (Montoya Díaz et al., 2012) when purchasing medicines. The assistance towards the cost of drugs is limited to specific diseases and treatments. In addition, two federal programs (Program for Sexually Transmitted Infections Treatment and Prevention, and the Program for the Dispensation of Special Medications for chronic conditions) provide assistance for costly medications. In 2012, one in four Brazilians had purchased an additional voluntary health plan or health insurance, but few of these covered costs of prescription drugs (Montoya Díaz et al., 2012).
Inequities persist in coverage of primary health care, with low coverage in the Northeast region and the Amazonian North, which have high levels of poverty, low-income levels, low educational attainment, high burden of communicable and non-communicable diseases, and segregation by race and ethnicity.
Employment, Retirement, and Workforce Productivity
Described as an “economic time bomb” (The Economist 2012), Brazil has 35 pensioners for every 100 contributing workers, and 13% of GDP is spent on pensions – more than any G7 country with the exception of Italy. This presents substantial challenges to Brazil as it faces an aging population with an increasing number of chronic conditions (Romero 2015).
Improvements in longevity bring challenges. In the 1950s, 90% of Brazilians aged 60-64 years were contributing to the workforce. In 2000, just 65% of the same age group remained in active employment. This shift was most evident in the public sector, which in 2002 had an average age of retirement and exit from employment of 52 years, compared to the official retirement age of 65 years for men and 60 years for women (Queiroz 2007). The average age of retirement across all sectors in Brazil is around 55 years (Queiroz, 2007).
Challenges in Productivity and Economic Growth
Productivity and investment are the cornerstones of economic growth. However, pension obligations and rapidly rising non-communicable diseases that bring chronic illness place a heavy burden on the government budget, reduce productivity, and limit economic growth in Brazil – which has experienced difficulty sustaining productivity growth, including total factor productivity, with declining investments as a proportion of GDP compared to other countries of South America (Palma, 2010).
Brazil needs greater public investment in cross-sectoral policies to improve health, education, and sustainable development – alongside pension reform – to boost productivity and address emerging adverse trends.
Turkey Case Study
During the 1990s, Turkey experienced political instability, an underperforming economy with rampant inflation, wide income inequalities, and few improvements in its health system (Atun et al., 2013). As a result, by the end of the 1990s, the Turkish health system faced major gaps in financial coverage and access to healthcare services. Only 66.3% of the population was covered by health insurance in 2003.
Inequitable and inadequate financing impeded access to health services for the poorest segments of the population who suffered impoverishing health expenditures, worsened by maldistribution and absolute shortage of human resources and infrastructures. As a result, although average life expectancy at birth increased through the 1990s, geographic and social inequities in health outcomes persisted (Atun et al., 2013).
To address the shortcomings in the health system and poor health outcomes, Turkey introduced the Health Transformation Program (HTP) in 2003. The HTP combined supply- and demand-side interventions to expand coverage of health financing and service delivery, enabled by economic growth that created the fiscal space to increase total health expenditures. Rapid scale-up of family medicine-centred primary health care was accompanied by expansion of health insurance coverage and the creation of a unified general health insurance system that brought together four separate health insurance schemes for blue-collar workers, civil servants, retired civil servants, and the self-employed, with aligned benefits for all population groups.
Contracts were used to source human resources for underprivileged areas of the country and to increase hospital capacity by engaging the private sector (Atun, 2015).
Health system reforms were effective in improving key health outcomes and providing financial protection, especially for the most disadvantaged population groups (Atun, 2015). Improved financial protection diminished catastrophic expenditures and contributed to poverty reduction at the national level. Although the evidence remains mixed, recent studies suggest a positive relation between increased health expenditures and economic growth in Turkey (Arisoy, Ünlükaplan, and Ergen, 2010; Kurt, 2015).
Health Outcomes, Socioeconomic Welfare, and Human Development
Maternal, child, and neonatal mortality are sensitive indicators of health system performance and are closely related to the availability of health resources (Dickson et al., 2014). In Turkey, between 1998 and 2009, neonatal mortality declined from 26 per 1,000 live births to 10 – a decline achieved by OECD countries in 30 years (Demirel et al., 2013). Infant and maternal mortality also declined (Baris et al., 2011; Atun et al., 2013).
Between 2000 and 2010, Turkey was ranked first among 113 low-income and middle-income countries in the rate of decline of under-five mortality (Verguet and Jamison, 2014). Between 2000 and 2008, average life expectancy at birth rose from 70 to 73 years (Baris, Mollahaliloglu, and Aydin, 2011). The HTP significantly reduced health inequities between different social groups (Atun et al., 2013).
Poverty Alleviation and Financial Protection
Expansion of the green card scheme led to an increase in insurance coverage for the poorest groups from 2.4 million in 2003 to 10.2 million people in 2011 (Ökem and Çakar, 2015). This enhanced financial protection led to a decrease in the share of out-of-pocket payments out of total health expenditures, especially for lowest-income households, and a decline in catastrophic health expenditures between 2003 and 2011 (Atun et al., 2013; Yardim et al., 2014).
Some studies argue that high-income groups benefited more from the decrease of out-of-pocket health expenditures (Erus and Aktakke, 2012), and between 2004 and 2010, the percentage of households who incurred catastrophic health expenditures may have increased (Özgen Narcı et al., 2015). While the HTP had a clear impact on financial and geographic equity, further studies are needed to eliminate regressive out-of-pocket patterns (Ökem and Çakar, 2015).
Health and Macroeconomic Growth
Studies examining the relationship between health expenditures and macroeconomic growth in Turkey since the 1960s show mixed results (Kurt, 2015). One study finds a positive impact of economic growth on total health expenditures, with a 10% increase in per capita GDP associated with an 8.7% increase in per capita health expenditures between 1984 and 2006 (Sulku and Bernard, 2012).
Two other studies suggest a positive impact of social and health investments on long-term macroeconomic growth: one study shows the positive effect of health and education expenditures on the Turkish economy for the period 1960-2005 (Arisoy, Ünlükaplan, and Ergen, 2010), and the other, which analyzes the impact of general government medicine and health expenditures on the Turkish economy between 2006 and 2013, finds a positive effect of government health expenditures on total expenditures, aggregate demand, and total production, and a negative impact of the expenditures in other sectors (Kurt, 2015).
Employment, Retirement, and Workforce Productivity
As with Brazil, the demographic and epidemiological shifts mean that Turkey faces a rapidly rising burden of non-communicable disease, an ageing population, and growing pension obligations. The rising chronic illness will place demands on the government health budget, and if not effectively managed, will have adverse consequences on population health outcomes, financial well-being, and economic growth.
To build on its success, Turkey needs to maintain the momentum in health systems reform and develop multisectoral policies to further strengthen primary health care and to establish a comprehensive set of services designed to prevent NCDs and effectively manage chronic illness (Atun et al., 2013).
Policy Implications
The three case studies from Ethiopia, Brazil, and Turkey examine the impact of investing in health systems on several health outcomes, economic growth, and sustainable development.
While the evaluation of the impact of the reforms is ongoing, direct and indirect effects of health investment in these countries are already apparent, with regards to improved health outcomes, financial protection, and poverty reduction.
Although implemented at different stages, and in different contexts, investments in health in these countries share several common characteristics:
Sustained political leadership: Political stability and sustained political leadership helped to introduce decisive and comprehensive reforms that combined social sector and health system reforms, with support across the government, which was crucial to achieve improvements in health, financial protection, improved economic growth, and development.
Effective use of fiscal space: The three countries used the fiscal space created by economic growth effectively to invest in the health system, especially in primary health care to improve coverage, efficiency, effectiveness, equity, and responsiveness of health services.
A transition towards universal health protection and coverage: Expanding access to health services and reducing catastrophic expenditures, especially for poor households, was an explicit goal of all three countries for improving financial protection.
An emphasis on developing strong primary health care: Although each country adopted a specific set of interventions, all placed a great emphasis on improving access to primary health care, either through the strengthening of family medicine, such as in Turkey, or through the expansion of decentralized primary health care in Ethiopia and Brazil with the use of health extension workers and community health workers.
A combination of supply- and demand-side interventions in the health system: As governments designed and implemented the reforms, policymakers recognized the need to simultaneously address both supply- and demand-side barriers to healthcare by introducing policies and interventions to stimulate demand and expand supply to enhance access to health services.
Though very successful, these countries face the rapidly growing burden of non-communicable diseases that will place demands on the government health budget. Judicious investments will be needed to develop strong health systems underpinned by comprehensive primary health care designed to manage chronic illness. Only then can the impressive achievements in health outcomes, poverty alleviation, and economic growth be sustained.
References
Acemoglu, Daron, and Simon Johnson. 2007. “Disease and Development: The Effect of Life Expectancy on Economic Growth.” Journal of Political Economy 115 (6): 925–85. doi:10.1086/529000.
Alkire, Sabina, Adriana Conconi, and Suman Seth. 2014. “Multidimensional Poverty Index 2014: Brief Methodological Note and Results.” Oxford: University of Oxford. Link.
Almond, Douglas. 2006. “Is the 1918 Influenza Pandemic Over? Long‐ Term Effects of In Utero Influenza Exposure in the Post‐ 1940 U.S. Population.” Journal of Political Economy 114 (4): 672–712. doi:10.1086/507154.
Almond, Douglas, Lena Edlund, and Mårten Palme. 2009. “Chernobyl’s Subclinical Legacy: Prenatal Exposure to Radioactive Fallout and School Outcomes in Sweden.” The Quarterly Journal of Economics 124 (4): 1729–72. doi:10.1162/qjec.2009.124.4.1729.
Arisoy, Ibrahim, Ilter Ünlükaplan, and Zuhal Ergen. 2010. “The Relationship between Social Expenditures and Economic Growth: A Dynamic Analysis Intended for 1960-2005 Period of the Turkish Economy.” Maliye Dergisi 158: 398–421.
Ashraf, Quamrul H., Ashley Lester, and David N. Weil. 2008. “When Does Improving Health Raise GDP?” Working Paper 14449. National Bureau of Economic Research. Link.
Atun, Rifat. 2015. “Transforming Turkey’s Health System — Lessons for Universal Coverage.” New England Journal of Medicine 373 (14): 1285–89. doi:10.1056/NEJMp1410433.
Atun, Rifat, Sabahattin Aydın, Sarbani Chakraborty, Safir Sümer, Meltem Aran, Ipek Gürol, Serpil Nazlıoğlu, et al. 2013. “Universal Health Coverage in Turkey: Enhancement of Equity.” The Lancet 382 (9886): 65–99. doi:10.1016/S0140-6736(13)61051-X.
Atun, Rifat, Luiz Odorico Monteiro de Andrade, Gisele Almeida, Daniel Cotlear, T. Dmytraczenko, Patricia Frenz, Patrícia Garcia, et al. 2015. “Health-System Reform and Universal Health Coverage in Latin America.” The Lancet 385 (9974): 1230–47. doi:10.1016/S0140-6736(14)61646-9.
Baris, Enis, Salih Mollahaliloglu, and Sabahattin Aydin. 2011. “Healthcare in Turkey: From Laggard to Leader.” BMJ 342 (January): c7456. doi:10.1136/bmj.c7456.
Bleakley, Hoyt. 2007. “Disease and Development: Evidence from Hookworm Eradication in the American South.” The Quarterly Journal of Economics 122 (1): 73–117. doi:10.1162/qjec.121.1.73.
Bloom, David E., and David Canning. 2000. “Population Health and Economic Growth.” Washington D.C.: World Bank Group. Link.
Bloom, David E., David Canning, and Günther Fink. 2014. “Disease and Development Revisited.” Journal of Political Economy 122 (6): 1355–66. doi:10.1086/677189.
Brandao Junior, Nilson, and Marianna Aragao. 2007. “Miséria No Brasil Cai 27,7% No 1o Mandato de Lula.” Estadão, September 20. Link.
Buckles, Kasey, Kasey Buckles, and Daniel M. Hungerman. 2008. “Season of Birth and Later Outcomes: Old Questions, New Answers.” NATIONAL BUREAU OF ECONOMIC RESEARCH (CAMBRIDGE, MA) WORKING PAPER. http://citeseerx.ist.psu.edu/viewdoc/summary?doi=10.1.1.584.9681.
Commission on Social Determinants of Health. 2008. “Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health.” Geneva: World Health Organization. Link.
Cutler, David, Winnie Fung, Michael Kremer, Monica Singhal, and Tom Vogl. 2010. “Early-Life Malaria Exposure and Adult Outcomes: Evidence from Malaria Eradication in India.” American Economic Journal: Applied Economics 2 (2): 72–94. doi:10.1257/app.2.2.72.
Deaton, Angus. 2003. “Health, Inequality, and Economic Development.” Journal of Economic Literature 41 (1): 113–58.
Deaton, Angus. 2006. “On Death and Money: History, Facts, and Explanations.” JAMA. Published online April 10, 2016. doi:10.1001/jama.2016.4072.
Demirel, Gamze, Basak Tezel, Sema Ozbas, Serife Suna Oguz, Omer Erdeve, Nurdan Uras, and Ugur Dilmen. 2013. “Rapid Decrease of Neonatal Mortality in Turkey.” Maternal and Child Health Journal 17 (7): 1215–21. doi:10.1007/s10995-012-1115-7.
Derseh, Anagaw, Robert Sparrow, Zelalem Debebe, Getnet Alemu, and Arjun Singh Bedi. 2013. “Enrolment in Ethiopia’s Community Based Health Insurance Scheme.” ISS Working Paper Series / General Series 578 (December): 1–35.
Dibaba, A, M Hadis, S Ababor, and Y Assefa. 2014. “Improving Health Care Financing in Ethiopia.” Addis Ababa: Ethiopian Public Health Institute. Link.
Dickson, Kim E, Aline Simen-Kapeu, Mary V Kinney, Luis Huicho, Linda Vesel, Eve Lackritz, Joseph de Graft Johnson, et al. 2014. “Every Newborn: Health-Systems Bottlenecks and Strategies to Accelerate Scale-up in Countries.” The Lancet 384 (9941): 438–54. doi:10.1016/S0140-6736(14)60582-1.
Erus, Burcay, and Nazli Aktakke. 2012. “Impact of Healthcare Reforms on out-of-Pocket Health Expenditures in Turkey for Public Insurees.” The European Journal of Health Economics: HEPAC: Health Economics in Prevention and Care 13 (3): 337–46. doi:10.1007/s10198-011-0306-2.
Ethiopian Health Insurance Agency. 2015. “Evaluation of Community-Based Health Insurance Pilot Schemes in Ethiopia: Final Report.” Addis Ababa: Ethiopian Health Insurance Agency. Link.
Ethiopia Federal Ministry of Health. April 2014. Ethiopia’s Fifth National Health Accounts 2010/2011. Addis Ababa, Ethiopia.
Field, Erica, Omar Robles, and Maximo Torero. 2009. “Iodine Deficiency and Schooling Attainment in Tanzania.” American Economic Journal: Applied Economics 1 (4): 140–69.
Floud, Roderick, Robert W Fogel, Bernard Harris, and Sok Chul Hong. 2011. The Changing Body: Health, Nutrition, and Human Development in the Western World since 1700. New York: Cambridge University Press. Link.
Fogel, Robert W. 1994. “Economic Growth, Population Theory, and Physiology: The Bearing of Long-Term Processes on the Making of Economic Policy” 84 (3): 369–95.
Galarraga O, Sosa-Rubi SG, Salinas-Rodriguez A, Sesma-Varquez S. 2010. “Health insurances for the poor: impact on catastrophic and out-of-pocket health expenditures in Mexico.” The European Journal of Health Economics 11 (5): 437-447.
Gallup, J. L., and J. D. Sachs. 2001. “The Economic Burden of Malaria.” The American Journal of Tropical Medicine and Hygiene 64 (1-2 Suppl): 85–96.
Health System Financing Reform Project. 2011. “Assessment of User Fee Revisions in Public Health Facilities in Ethiopia: SNNP Regional Report.” Hawassa: USAID.
HEPCAPS11 Project Team 2. 2012. “Developing Primary Health Care Delivery in Lower and Middle Income Countries: Challenges Faced and Lessons Learned.” Boston, MA, and New Haven, CT: Harvard School of Public Health and Global Health Leadership Institute at Yale University.
IHME. 2013. “Country Profiles.” Seattle: Institute for Health Metrics and Evaluation.
Jamison, Dean T., Lawrence H. Summers, George Alleyne, Kenneth J. Arrow, Seth Berkley, Agnes Binagwaho, Flavia Bustreo, et al. 2013. “Global Health 2035: A World Converging within a Generation.” Lancet (London, England) 382 (9908): 1898–1955. doi:10.1016/S0140-6736(13)62105-4.
Knaul, Felicia Marie, Rebeca Wong, Héctor Arreola-Ornelas, Oscar Méndez, and Network on Health Financing and Social Protection in Latin America and the Caribbean (LANET). 2011. “Household Catastrophic Health Expenditures: A Comparative Analysis of Twelve Latin American and Caribbean Countries.” Salud Pública De México 53 Suppl 2: s85–95.
Kremer, Michael, Jessica Leino, Edward Miguel, and Alix Peterson Zwane. 2011. “Spring Cleaning: Rural Water Impacts, Valuation, and Property Rights Institutions*.” The Quarterly Journal of Economics 126 (1): 145–205. doi:10.1093/qje/qjq010.
Kurt, Serdar. 2015. “Government Health Expenditures and Economic Growth: A Feder–Ram Approach for the Case of Turkey.” International Journal of Economics and Financial Issues 5 (2): 441–47.
Lagarde M, Palmer N. “The impact of user fees on health service utilization in low- and middle-income countries: how strong is the evidence?” Bulletin of the World Health Organization 86: 839-848.
Lucas, Adrienne M. 2010. “Malaria Eradication and Educational Attainment: Evidence from Paraguay and Sri Lanka.” American Economic Journal: Applied Economics 2 (2): 46–71. doi:10.1257/app.2.2.46.
Miguel, Edward, and Michael Kremer. 2004. “Worms: Identifying Impacts on Education and Health in the Presence of Treatment Externalities.” Econometrica 72 (1): 159–217. doi:10.1111/j.1468-0262.2004.00481.x.
Monteiro de Andrade LO, Filho AP, Solar O, Rigoli F, Malagon de Salazar L, Castell-Florit Serrate P, Ribeiro KG, Swift Koller T, Bravo Cruz FN, Atun R. 2015. “Social determinants of health, universal health coverage, and sustainable development: case studies from Latin American countries.” The Lancet 385 (9975): 1343-1351.
Montoya Díaz, María Dolores, Flavia Mori Sarti, Antonio Carlos Coelho Campino, and Roberto Iunes. 2012. “Catastrophic Health Expenditure in Brazil: Regional Differences, Budget Constraints and Private Health Insurance.” In Financing Health in Latin America, Volume 1: Household Spending and Impoverishment, edited by Felicia Marie Knaul, Rebeca Wong, and Héctor Arreola-Ornelas, 111–26. Cambridge, MA: Harvard University Press. Link.
National Population and Housing Census of Ethiopia. 2007. Addis Ababa, Ethiopia. Link.
Newhouse JP. 1993. “Free for All? Lessons from the RAND Health Insurance Experiment”. Cambridge: Harvard University Press. Link.
Ökem, Zeynep Güldem, and Mehmet Çakar. 2015. “What Have Health Care Reforms Achieved in Turkey? An Appraisal of the ‘Health Transformation Programme.’” Health Policy 119 (9): 1153–63. doi:10.1016/j.healthpol.2015.06.003.
Özgen Narcı, Hacer, İsmet Şahin, and Hasan Hüseyin Yıldırım. 2015. “Financial Catastrophe and Poverty Impacts of out-of-Pocket Health Payments in Turkey.” The European Journal of Health Economics: HEPAC: Health Economics in Prevention and Care 16 (3): 255–70. doi:10.1007/s10198-014-0570-z.
Paes-Sousa, Romulo. 2013. “New Strategy for Poverty Eradication in Brazil: The Emergence of the Brasil Sem Miséria Plan.” 214. Brasilia: International Policy Centre for Inclusive Growth. Link.
Paim, Jairnilson, Claudia Travassos, Celia Almeida, Ligia Bahia, and James Macinko. 2011. “The Brazilian Health System: History, Advances, and Challenges.” Lancet (London, England) 377 (9779): 1778–97. doi:10.1016/S0140-6736(11)60054-8.
Palma, José Gabriel. 2010. “Why Has Productivity Growth Stagnated in Most Latin American Countries since the Neo-Liberal Reforms?” Cambridge: University of Cambridge. Link.
Queiroz, Bernardo Lanza. 2007. “The Determinants of Male Retirement in Urban Brazil.” Nova Economia 17 (1): 11–36. doi:10.1590/S0103-63512007000100001.
Romero, Simon. 2015. “An Exploding Pension Crisis Feeds Brazil’s Political Turmoil.” The New York Times, October 20. Link.
Sachs, JD. 2001. “Macroeconomics and Health: Investing in Health for Economic Development.” Report of the Commission on Macroeconomics and Health. Geneva: World Health Organization. Link.
Siroka A, Ponce NA, Lönnroth K. 2015. “Association between spending on social protection and tuberculosis burden: a global analysis.” The Lancet Infectious Diseases 16 (4): 473-479.
Somkotra T, Lagrada LP. 2009. “Which households are at risk of catastrophic health spending: experience in Thailand after universal coverage.” Health Affairs 28 (3): 467-478.
Strauss, John, and Duncan Thomas. 1998. “Health, Nutrition, and Economic Development.” Journal of Economic Literature 36 (2): 766–817.
Sulku, S Nur, and D Minbay Bernard. 2012. “Financial Burden of Health Care Expenditures: Turkey.” Iranian Journal of Public Health 41 (3): 48–64.
The Economist. 2012. “Tick, Tock.” The Economist, March 24. Link.
The Ethiopian Federal Ministry of Health. 2010. “Ethiopia’s Fourth National Health Accounts, 2007/2008.” Addis Ababa: The Ethiopian Federal Ministry of Health.
———. 2011. “Health and Health Related Indicators for 2003 EC (2011 GC).” Addis Ababa: The Ethiopian Federal Ministry of Health.
Thomas, Duncan, Elizabeth Frankenberg, Jed Friedman, Jean-Pierre Habicht, Mohammed Hakimi, Nathan Jones, Christopher McKelvey, et al. 2003. “Iron Deficiency and the Well-Being of Older Adults: Early Results from a Randomized Nutrition Intervention.” In . San Francisco. Link.
USAID. 2011. “Ethiopia Health Sector Financing Reform Midterm Project Evaluation.” Washington D.C.: USAID. Link.
Verguet, Stéphane, and Dean T. Jamison. 2014. “Estimates of Performance in the Rate of Decline of under-Five Mortality for 113 Low- and Middle-Income Countries, 1970-2010.” Health Policy and Planning 29 (2): 151–63. doi:10.1093/heapol/czs143.
Wagstaff, Adam. 1987. “Government Prevention Policy and the Relevance of Social Cost Estimates.” British Journal of Addiction 82 (5): 461–67. doi:10.1111/j.1360-0443.1987.tb01502.x.
———. 2008. “Measuring Financial Protection in Health.” SSRN Scholarly Paper ID 1106043. Rochester, NY: Social Science Research Network. Link.
Wagstaff, Adam, and Eddy van Doorslaer. 2003. “Catastrophe and Impoverishment in Paying for Health Care: With Applications to Vietnam 1993-1998.” Health Economics 12 (11): 921–34. doi:10.1002/hec.776.
Whitehead, M, and G Dahlgren. 1991. “What Can Be Done about Inequalities in Health?” The Lancet 338 (8774): 1059–63. doi:10.1016/0140-6736(91)91911-D.
WHO. 1999. “The World Health Report 1999: Making a Difference.” Geneva: World Health Organization. Link.
———. 2000. “The World Health Report 2000 – Health Systems: Improving Performance.” Geneva: World Health Organization. Link.
———. 2010. “The World Health Report: Health Systems Financing, the Path to Universal Coverage.” Geneva: World Health Organization. Link.
———. 2016. “Global Health Expenditures Database.” Geneva: World Health Organization. Link.
World Bank. 2015. “Ethiopia Poverty Assessment 2014.” Washington D.C.: World Bank Group. Link.
———. 2016. “World Development Indicators.” February 16. Link.
Yardim MS, Cilingiroglu N, Yardim N. 2010. “Catastrophic health expenditure and impoverishment in Turkey.” Health Policy 94 (1): 26-33.
Xu, Ke, David B. Evans, Kei Kawabata, Riadh Zeramdini, Jan Klavus, and Christopher J. L. Murray. 2003. “Household Catastrophic Health Expenditure: A Multicountry Analysis.” Lancet (London, England) 362 (9378): 111–17. doi:10.1016/S0140-6736(03)13861-5.
Appendix
Table 3. Socioeconomic Data (Source: World Bank Open Data, 2014)
Argentina
Brazil
Chile
Colombia
Mexico
Peru
Venezuela*
GDP (US$, billions)
537.7
2,346.1
258.1
377.7
1,294.7
202.6
381.3
GDP (US$, per capita)
12,509.5
11,384.4
14,528.3
7,903.9
10,325.6
6,541.0
12,771.6
Health Spending (US$, per capita)
1,074
1,085
1,204
533
664
354
520
Total Health Expenditure (%GDP) *
7.3
9.7
7.7
6.8
6.2
5.3
3.6
Out-of-Pocket Health Expenditure (%THE) *
21.1
29.9
31.7
13.9
44.1
34.9
65.8
Literacy (Female %)
98
92
97
94
93
91
95
Literacy (Male %)
98
91
97
93
95
97
95
Life Expectancy at Birth (Female)
79.6
78.4
81.7
78.9
78.7
78.7
79.3
Life Expectancy at Birth (Male)
72.3
71.6
76.3
72.3
72.2
75.5
71.8
Life Expectancy at 50 Years (Female)
32.3
31.6
33.5
32.0
31.7
32.0
32.2
Life Expectancy at 50 Years (Male)
26.4
27.5
29.5
28.4
27.7
30.0
28.1
Health-Adjusted Life Years at Birth (Female)
69.4
67.0
70.8
67.6
67.8
67.2
68.2
Health-Adjusted Life Years at Birth (Male)
64.2
62.8
67.3
63.2
63.8
65.0
63.3
Source: World Bank Open Data, 2014. All US$ current prices, unless otherwise stated. Available online: http://data.worldbank.org/
Life expectancy data source: Institute for Health Metrics and Evaluation, 2013. Asterisk * represents data from 2012-2013.
Rifat Atun, Claire Chaumont, Joseph R Fitchett, Annie Haakenstad, Donald Kaberuka.
Harvard T.H. Chan School of Public Health, Harvard University, Boston, MA 02215, USA
John F. Kennedy School of Government, Harvard University, Cambridge, MA 02138, USA
Education, general health, and reproductive health (RH) are widely understood to be key indicators of human development. Investments in these domains can also promote economic growth by enhancing worker productivity and labor supply, and inducing higher rates of saving, capital accumulation, and technological progress. While substantial evidence supports the impact of human development on economic growth, economic literature does not provide any clear indications with regard to which aspects of human development have the most potent influences on economic growth. The literature also fails to provide a clear comparison of the importance of human development and its components relative to other drivers of growth, such as those related to institutional quality, macroeconomic management, or the nature and density of infrastructure.
This paper seeks to summarize the literature on the returns to different human development strategies and to provide original empirical evidence on the relative impact of improvements in different aspects of human development on subsequent economic growth. It also offers guidance on prioritizing expenditures within sector by reviewing literature on the social and private returns to different education, health, and reproductive health interventions.
Cross-country Differences in Economic Performance
Most countries classified as low- or middle-income in the mid-20th century experienced substantial economic growth over the last 70 years, but average incomes have improved considerably more in some countries than others. These growth discrepancies are most evident when one contrasts the economic growth experience of East Asia with that of sub-Saharan Africa. In 1960, both regions had comparable per capita GDP. But real income in East Asia grew to more than 800% of its 1960 value by 2017, whereas income per capita in sub-Saharan Africa grew by only 50% over the same period (see Figure ES1).
Figure ES1. Real GDP per capita of LMICs in 1960 and 20172 with linear projections by region
Cross-country differences in rates of income growth have been accompanied by corresponding differences in trajectories of human development, especially in education, life expectancy, and fertility (see Table ES1).
Table ES1. Income and Indicators of Human Development by Current Income Grouping
Variable
1990 Value
2017 Value
Change (%)
Low-Income Countries
Income p.c. (in 2010 US$)
567
720
27
Life Expectancy at Birth
51
63
24
Literacy Rate (Age 15+)
46
61
33
Total Fertility Rate (TFR)
6.3
4.6
-27
Lower-Middle-Income Countries
Income p.c. (in 2010 US$)
944
2,189
132
Life Expectancy at Birth
59
68
15
Literacy Rate (Age 15+)
58
76
31
Total Fertility Rate (TFR)
4.9
2.8
-33
Upper-Middle-Income Countries
Income p.c. (in 2010 US$)
3,148
8,225
161
Life Expectancy at Birth
69
75
9
Literacy Rate (Age 15+)
82
95
16
Total Fertility Rate (TFR)
2.6
1.8
-31
2 The general patterns shown in this chart also hold for purchasing power parity (PPP) adjusted GDP, although PPP-adjusted data are only available from 1990 onward.
The association between these human development outcomes and economic growth is consistent with economic theory and presumably reflects a bi-causal relationship: (i) the extent to which increased income allows individuals and governments to invest more heavily in human development, and (ii) the impact of improvements in general health, reproductive health, and education on economic growth.
Variation in Resource Allocation
Expenditures on health and education, as well as those on infrastructure, vary appreciably across LMICs. Across the entire LMIC group, health expenditures range from less than 3% of GDP in Bangladesh, Pakistan, and Angola to more than 9% in Uruguay, Malawi, and Serbia. Education expenditures range from below 3% of GDP in South Sudan, Sri Lanka, and Kazakhstan to more than 7% in Costa Rica, Senegal and Bhutan.3 The lowest-income countries have tended to increase expenditures on health, education, and infrastructure more rapidly in recent years than upper-middle income countries [see Table A4]. Increases in these expenditures are all associated with more rapid GDP growth in subsequent years [see Figures A5-A7].
Literature on Drivers of Economic Growth
Theoretical considerations and empirical evidence strongly support the conclusion that the positive association between expenditures on human development and the pace of economic growth reflects at least partially, a causal impact of improved general health, reproductive health, and education on economic growth. By contrast, evidence that infrastructure investments drive economic growth is less clear cut.
There are several pathways through which education can contribute to increased economic growth. Better educated workers: (i) are more productive, (ii) are more likely to participate in the labor force, (iii) tend to have longer working lives, (iv) are more likely to establish successful and productive firms, (v) more readily adopt and more efficiently assimilate technologies from abroad, and (vi) enhance the productivity of their co-workers through beneficial synergies and spillovers.
Results suggest that, on average, individual income is 10% higher for each additional year of schooling received. Some results estimate even higher returns for low-income countries. Average private rates of return to schooling are highest in Latin America and the Caribbean and for sub-Saharan Africa, and lowest for Europe and the Middle East and Northern Africa. Recent literature suggests that the rate of return to education increases considerably (from 11% to 16%) if the impacts of education on mortality are taken into account. Furthermore, a large body of macroeconomic literature finds education to be a key determinant of economic growth and suggests that the impact of education on individual productivity aggregates up to greater total productivity at the country level – perhaps because of beneficial spillovers among a more educated workforce and because such a workforce attracts more foreign direct investment. In general, the literature suggests that a one-year increase in average educational attainment is associated with between a 0.5 and 1.2 percentage point (pp) increase in the annual growth rate of GDP per capita. A 25 point improvement in PISA score,4 a measure of educational quality, is similarly associated with a 0.5 pp increase in annual GDP per capita growth.
A substantial body of literature finds consistent patterns in the returns to different types of educational investment. Investments in primary education generally offer higher returns than those in secondary education and tertiary education (see Table ES2). Investing in high quality pre-primary education can also have huge positive returns, even in very low-income settings. Returns to girls’ education are generally higher than those for boys’ education and have important economically beneficial spillover effects through reducing the TFR and promoting stronger families and communities. This is particularly the case in settings with large gender gaps in educational attainment.
3 Even among settings in which expenditures are comparable as a share of GDP, per capita expenditures vary substantially. For example, 9% of GDP per capita is roughly US$530 in Serbia but only US$30 in Malawi.
4 This 25 point improvement in PISA score is relative to a normalized mean of 500 and standard deviation of 100.
Table ES2. Social returns to investments in education, 1960-2014
Low income
Middle income
Primary
22.08%
17.10%
Secondary
18.10%
12.79%
Tertiary
13.18%
11.44%
Source: Meta-study of Psacharopoulos and Patrinos (2018)
Investments in health also enhance productivity and economic growth through several channels: (i) healthier workers tend to be more consistently working and more productive when working; (ii) healthier children tend to perform better in school, attend school for more years, and accumulate more human capital in the process, which tends to enhance their productivity and incomes in adulthood, (iii) healthier individuals have greater incentive to pursue education and save for retirement, (iv) healthy populations are more powerful attractors of foreign direct investment, and (v) health investments that cure or prevent infectious diseases (such as vaccination) have positive spillovers to other individuals.
Here, too, the positive effects of improved health on individual productivity are consistent with macro-level evidence suggesting that health is an important determinant of economic growth. Estimates from the literature suggest that a 10% increase in the adult survival rate leads to a 6.7% increase in productivity per worker and a 4.4% increase in GDP per worker. Other research estimates that, on average, a one-year increase in life expectancy at birth causes a 4% increase GDP per capita.
In addition to enhancing productivity, investments in education and health facilitate escape from the often crushing burden of youth dependency. Poor countries tend to have much higher youth dependency rates than wealthier countries. Supporting the basic needs of a relatively large child population imposes a substantial resource burden, necessitating the diversion of resources from other productive investments and impeding, for decades, the pace of measured economic growth. As child survival improves, and as women become healthier, more educated, and more empowered, desired fertility tends to decline. Major drops in fertility initiate a period of lower youth dependency, during which resources are freed up for other productive investments. If properly harnessed, this fertility transition can result in a sizable boost to economic growth, known as the “demographic dividend”.
Results from the literature imply that a fall in the TFR by one child leads to an economic growth rate that is 0.45 pp higher. Other analyses suggest that one-third of East Asia’s “growth miracle” is due to the demographic dividend that followed the strong decline in fertility in China, South Korea, Hong Kong, Singapore, and Taiwan. This one-third figure corresponds to a 0.66 pp increase in the growth rate of per capita GDP for each one-child reduction in the TFR.
Results from the literature are mixed with respect to infrastructure spending. Some results suggest that government consumption, particularly in the form of spending on infrastructure, serves to enhance economic development and growth. Other studies find no effect, which may reflect the fact that private investment is crowded out by spending on public infrastructure.
Empirical Analyses
This report presents original empirical analysis in the form of single and multiple equilibria cross-sectional and panel growth regressions. Multiple equilibria models are able to account for the fact that the variables of interest may have distinct effects on economic growth in developing and developed countries (defined both in terms of income group and timing of demographic transition). Whereas the cross-section threshold growth regressions focus on the long-run effects, dynamic panel threshold regressions allow us to instrument the independent variables and perform an improved causal inference over shorter (i.e., five-year) intervals from 1980 through 2015. The aim is to estimate the impact of different health, fertility, education, and infrastructure indicators on GDP per capita growth simultaneously and under an internally consistent methodological framework.
We contrast these results with those summarized from the extant literature , which are typically based on a variety of sources that make use of different country samples, time frames, controls, and datasets (of varying quality). Earlier studies also utilize different econometric methods and take different types of costs and benefits into account. While these results are helpful for discerning the general economic impacts of improvements in specific outcomes, they do not lend themselves easily to straightforward comparisons of impacts of different types of outcomes on economic growth.
Taken as a whole, our empirical analyses suggest four main findings relevant to policymakers in LMIC settings:5
A sustained one-child decrease in the TFR corresponds to a 2 pp increase in annual GDP per capita growth in the short-run (5 years) and 0.5 pp higher annual growth in the medium- to long-run (35 years).
A 10 percent increase in life expectancy at birth6 corresponds to a 1 pp increase in annual GDP per capita growth in the short-run and 0.4 pp higher growth in the medium- to long-run.
A one-year increase in average educational attainment corresponds to a 0.7 pp increase in annual growth in the short-run and 0.3 pp higher growth in the medium- to long-run.
Infrastructure proxies were not significantly associated with subsequent growth in any of the models whose parameters we estimated.
5 The relationships between these variables likely vary with contextual factors. As such, the results presented should be understood as average, at-the-margin, estimates. Additionally, as mentioned above and described in the main body of this manuscript, different methodologies are used to estimate short-run and mid- to long-run effects, so conclusions about the timeline of the return on benefits should be made cautiously
6 This is equal to a 6.3-year increase in life expectancy at birth for the average low-income country, a 6.8-year increase for the average lower-middle-income country, and a 7.5-year increase for the average upper-middleincome country.
Given that per capita GDP growth in LMICs generally averages between 2 and 4 pp, the estimated changes in annual growth provided above are appreciable. In interpreting these results, it is important to consider the compounding effect of a persistent change in growth over several years. For example, a 1 pp increase in average annual economic growth from 3% to 4% cumulates to GDP per capita that is 3.9 times higher after a period of 35 years rather than 2.8 times higher.
Prioritizing Expenditures within Sector: Copenhagen Consensus Findings
Additional results from the literature offer guidance on prioritizing expenditures within given sectors (for example, on the highest return health investments). The Copenhagen Consensus (CC) Center’s Post-2015 Consensus Project brought together economists and experts from the UN, NGOs, the private sector, and the academic community to produce over 100 literature- and evidence-informed reports on the effectiveness of the development targets proposed by the UN’s Open Working Group. The group of reports were reviewed by an expert panel that prioritized the goals according to the value offered per dollar spent attaining them.
The aggregated research results of the Post-2015 Consensus priorities rank the returns to one US dollar spent from 2015 to 2030 on meeting the UN-proposed development targets. The list of top-ranked outcomes, provided in Table ES3, highlights specific targets within general health, reproductive health, education, and other domains that merit particular focus.7 It is worth noting that these recommended targets are highly consistent with our empirical findings; improving access to reproductive health tops the list and the majority of other outcomes are health-related.
Many of the CC’s recommendations have proven fairly stable over time: increasing availability of family planning, reducing under-nutrition among preschoolers, expanding access to tuberculosis treatment, promoting malaria prevention and treatment, and providing aspirin to reduce heart attack risk all ranked among the top 20 interventions in the previous two lists of CC recommendations released in 2008 and 2012.
7 For the health-focused studies mentioned below, the returns refer to the discounted value of gains in disabilityadjusted life years relative to the actual costs of the intervention.
Table ES3. Top 10 post-2015 Consensus priorities
Category
Sub-category
Ratio of Returns to Investment
Reproductive health
Universal access to sexual and reproductive health (SRH)
120
Nutrition
Reduce by 40 per cent the number of children under 5 who are stunted
60
Illicit financial flows
Reduce to zero
49
Population and Demography
Reduce barriers to migration within low- and middle-income countries, as well as between low- and middle-income countries and high-income countries
45
Health
Reduce Tuberculosis deaths by 95% and TB incidence by 90%
43
Health
Delay artemisinin resistance and reduce malaria incidence using bed nets by 50%
36
Food security
Increase investment in agricultural R&D by 160%
34
Education
Increase the preschool enrollment ratio in sub-Saharan Africa from the present 18% to 59%
33
Health
Aspirin therapy at the onset of AMI (75% coverage)
31
Health
In hyper-endemic countries, attain circumcision coverage of at least 90% amongst HIV-negative adult men
28
Conclusions
Taken as a whole, economic theory, empirical literature on returns to spending on interventions
aimed at promoting different aspects of human development, and new evidence on the drivers
of economic growth suggest the following 3 conclusions:
Reducing fertility has considerable potential to boost the rate of economic growth, especially in settings in which fertility remains well above replacement. Reduced fertility offers very large economic returns over the short- and medium-long-run that are highly robust to different estimation and measurement methodologies.
Improving general health and education also promote economic growth. Improvements in health will have a more appreciable impact on economic growth in settings in which health is initially very poor, while education is relatively more potent in settings characterized by moderately good health.
Infrastructure gains do not show a consistent relationship with economic growth in the literature and are not significantly associated with economic growth in our analyses.8 This suggests that the capacity of infrastructure projects to improve economic growth should be evaluated on a case-by-case basis.
Concluding Caveats
The results presented herein refer to average effects associated with improvements in different
human development indicators, with little attention to the distribution of benefits across settings
and interventions. For example, a program to expand access to birth control may be highly
successful in reducing fertility in a locality where unmet need for contraceptives is high, but
completely ineffective in another environment where individuals desire a large number of
offspring. As such, policymakers must consider the specific binding constraints to development in their settings, as well as the relative cost of the options available for achieving improvements in health, education, fertility, and infrastructure, in order to make sound assessments of their relative returns on investment (ROIs). Ultimately, the rational allocation of resources to different interventions remains highly contextual, and will also be driven by whether decision-making exercises are aimed at allocating fixed sectoral budgets, or at determining the socially optimal size of a sectoral budget as well. Evidence-based resource allocation decisions seem advisable, but it should also be noted that the evidence is very thin with respect to (a) whether, for example, doubling the improvement in some human development indicator more than or less than or exactly doubles the ensuing boost to economic growth; (b) the likely existence of positive and negative interactions among different interventions (presumably because they are so difficult to tease out from existing data); and (c) the time frames in which income benefits are realized, which will naturally vary according to the nature of the human development investment, with the most immediate benefits coming from fertility decline and the most delayed benefits being associated with improvements in child health.
8 While the absence of a significant relationship is to some extent consistent with the theory of poverty traps, it could also be explained as a result of lack of impact of the projects themselves, the inadequacy of indicators used to proxy infrastructure quality, or the possibility that infrastructure financing effectively crowds out equallybeneficial private sector investments.
0. Prioritizing governmental expenditures: research results and guidance for policymakers
1. Introduction
Most countries classified as low- and middle-income at the mid-20th century experienced substantial economic growth over the last 70 years but this rising tide has lifted some countries far higher than others. These growth discrepancies are exemplified by contrasting the
experience of East Asia, where real per capita income grew to more than 8 times its 1960 value by 2017, with that of sub-Saharan Africa, where income increased by only around 50% over the same period (See Figure 1). This divergence in income has been accompanied by a divergence in human development, notably through stark differences in education, life expectancy, and fertility (see Table 1).
Figure 1. Real GDP per capita of LMICs in 1960 and 2017 with Regional Projections
Source: World Bank (2018)
Table 1. Income and Indicators of Human Development by Current Income Grouping
Variable
1990 Value
Current Value
Change (%)
Low-Income Countries
Income (in 2010 US$)
567
720
27
Life Expectancy at Birth
51
63
24
Literacy Rate (Age 15+)
46
61
33
Total Fertility Rate (TFR)
6.3
4.6
-27
Lower-Middle-Income Countries
Income (in 2010 US$)
944
2,189
132
Life Expectancy at Birth
59
68
15
Literacy Rate (Age 15+)
58
76
31
Total Fertility Rate (TFR)
4.9
2.8
-33
Upper-Middle-Income Countries
Income (in 2010 US$)
3,148
8,225
161
Life Expectancy at Birth
69
75
9
Literacy Rate (Age 15+)
82
95
16
Total Fertility Rate (TFR)
2.6
1.8
-31
An abundance of evidence supports the notion that different aspects of human development are strongly and reliably associated with economic growth (Ranis, 2004; Suri et al., 2011; Deaton, 2008). Although economic growth does not guarantee improved living conditions—if, for example, additional income is distributed in a highly disparate fashion or misdirected—an expansion of resources allows both individuals and governments the opportunity to invest more heavily in areas that directly impact wellbeing. International experience suggests that growth is vital to aiming beyond “low-bar” development goals, related to eliminating extreme poverty, towards achieving higher standards of well-being (Pritchett & Kenny, 2013). As such, policymakers and other stakeholdersinterested in promoting human development would benefit from a better understanding of the factors that have contributed to the divergent growth of LMICs in the last century, especially those factors that they can influence. Economic prioritization could subsequently offer an additional guideline for international organizations focused on providing foreign aid.9
Furthermore, much of the evidence regarding the relationship between economic growth and human development points to the importance of human capital, technology, and demographic variables as drivers of growth (Barro, 2001; Hanushek, 2013; Bloom & Canning, 2000; Malecki, 1997; Bloom, Canning, & Malaney, 2000; Lee & Mason, 2010). Accordingly, it is now widely appreciated that efforts to improve health, education, and access to family planning are, in fact, supportive of economic growth.
However, the relative prioritization of health, education, and infrastructure varies considerably across LMICs, as reflected by cross-country differences in spending on these sectors. Health expenditures, for example, range from less than 3% of GDP in Bangladesh, Pakistan, and Angola to more than 9% in Uruguay, Malawi, and Serbia. Education expenditures range from below 3% of GDP in South Sudan, Sri Lanka, and Kazakhstan to more than 7% in Costa Rica, Senegal and Bhutan. While the variation between countries is substantial, the average levels of spending (as a percentage of GDP) are actually fairly consistent across income groups; on average, upper-middle income countries spend only a modest share more on health and education than the lowest-income countries [see Table A3].10 Nonetheless, increases in these expenditures at the country-level are associated with more rapid GDP growth in subsequent years [see Figures A5-A7].
Substantial theory and evidence suggests that the association between these increased expenditures and faster economic growth reflects, at least partially, the causal impact of improved health and education on economic growth. Nonetheless, the information available in the literature does not yield an immediate conclusion as to which of these investments convey the biggest boost to economic growth. It also does not provide a clear comparison of the importance of these variables relative to other drivers of growth, such as trade, institutions, macroeconomic policy, or infrastructure.
This paper offers a basis for prioritizing different forms of development expenditure by drawing on evidence from low- and middle income countries (LMICs) on the association between different investment strategies and subsequent growth trajectories. It also offers guidance on prioritizing expenditures within sector by presenting information from the literature on which education, health, and reproductive health interventions have the biggest impacts on economic growth and development. A review of existing literature is used to inform priority setting within and across sectors and original empirical analysis is used to provide additional information on priority setting across sectors. In this analysis, we deliberately abstract from the other beneficial effects offered by health, education, and lower fertility rates.11 As such, the impacts on economic growth described in the paper should be considered in complement with the various other benefits resulting from spending in a given domain or on a specific program.
The manuscript is organized as follows: Section 2 describes a theoretical framework motivating the importance of large-scale investment in physical or human capital to escaping national poverty traps. Section 3 provides a literature review on the causal pathways from health, education, and fertility to economic growth, and the evidence supporting these mechanisms. Section 4 describes the methodological approach taken in this paper to assess the impacts of health, education, and demographic variables on economic growth, and presents the results of these analyses. Section 5 provides guidance on economic prioritization between and within sectors, Section 6 offers information on prioritization with respect to the Copenhagen Consensus, and Section 7 concludes.
9 Analysts offer a wide range of opinions on the effects of foreign aid: from little to no effects (Burnside and Dollar, 2000 and Easterly et al. 2004) to the transformational impulse of the big push (see Sachs, 2005).
10Even among settings in which expenditures are comparable as a share of GDP, per capita expenditures vary substantially.
For example, 9% of GDP per capita is roughly US$530 in Serbia but only US$30 in Malawi.
11For example, we do not consider the direct impact of increased life expectancy on improving welfare, which greatly exceeds the indirect effects of health on economic growth (Kuhn and Prettner, 2016; Baldanzi et al. 2019; Fan et al., 2018).
2. Theoretical Analysis
To illustrate the differential effects of investments in infrastructure, health, education, and fertility reduction from a qualitative point of view, we consider an economy in which time 𝑡 = 1,2 … evolves discretely. Aggregate output 𝑌t depends on the stocks of physical capital 𝐾t and human capital 𝐻t employed in the production process. These two accumulable production factors can be combined to produce aggregate output according to the overall productivity level 𝐴t. The production function that translates factor inputs and productivity into output has the general form 𝑌t = 𝐹(𝐴t, 𝐾t, 𝐻t), where 𝐹(… ) has positive first partial derivatives and negative second partial derivatives with respect to the accumulable production factors 𝐾t and 𝐻t. Physical capital comprises private production capital such as machines, production halls, and office buildings, but also public capital such as railroads, highways, electricity grids, and ports. In contrast to physical capital, human capital is embodied in the workers of an economy and is mainly determined by the average health status and education level of the workforce. Productivity 𝐴t consists of two parts: the technological state of the economy determining the location of the production possibility frontier, and the efficiency of input use determining whether the economy produces at its production possibility frontier (is efficient) or below its production possibility frontier (is inefficient).
2.1 The case of a unique steady-state equilibrium
In a perfectly competitive economy with full information and without externalities, the investment decisions of all agents are efficient. The private rate of return and social rate of return coincide for each investment such that the equilibrium outcome is optimal and does not require governmental intervention. In this case, the economy develops according to the well-known dynamics of standard economic growth models with exogenously increasing technology (cf. Solow, 1956; Diamond, 1965). We illustrate the development process of such an economy in Figure 2. The horizontal axis depicts the physical capital stock at time 𝑡, while the vertical axis refers to the physical capital stock at time 𝑡 + 1. The capital stock in each period is carried over from the previous period net of the depreciation of old capital, as given by 𝛿 ∗ 𝐾t (where 𝛿 is the depreciation rate). The capital stock rises because of gross investment 𝐼t = 𝑠 ∗ 𝐹(𝐴t, 𝐾t, 𝐻t) (where 𝑠 is the saving rate).
For this illustration, we assume that productivity and human capital stay constant at the levels 𝐴̅ and 𝐻̅ and that the function 𝐹(𝐴̅, 𝐾t, 𝐻̅) is concave in 𝐾t because the marginal product of physical capital is diminishing. Thus, at some point, capital accumulation stops because additional gross investment is only sufficient to replace additional depreciation. If this is the case, the capital stock at time 𝑡 and the capital stock at time 𝑡 + 1 coincide and the economy is at its steady state. In Figure 2, this point is the intersection of the 𝐾t+1-curve and the 45° line at the corresponding steady-state capital stock 𝐾*. At this steady state, the economy is comparatively rich. Output growth at the long-run steady state depends mainly on technological progress that shifts the production possibility frontier outwards (Romer, 1990). In empirical analyses of long-run growth processes in developed countries, the determinants of technological progress are the main regressors of interest, and the specifications of the growth regressions are typically standard linear models of either a cross-country or panel data structure.
Figure 2. Economic development based on capital accumulation without a poverty trap. The figure illustrates the growth process as described by a discrete-time version of the Solow (1956) model with a constant human capital stock and constant technology.
2.2 The case of multiple equilibria and poverty traps
In contrast to the case of a unique steady-state equilibrium in high-income countries, market imperfections, externalities, and coordination failures between different agents might imply the presence of multiple steady-state equilibria in low-income countries. The multiplicity of equilibria means that some economies will be caught in a poverty trap. In such a poverty trap, income is much lower than it could be at the high-income steady state (described in the previous paragraph) because endogenous forces push the economy back into a low-income equilibrium.
Two potential mechanisms that sustain poverty traps are:
Health: The general health status of the population could be very low due to widespread infectious diseases. Consequently, life expectancy might be so low that private investments in education do not pay off (Ben-Porath, 1967; Cervellati and Sunde, 2005, 2013). In this situation, building schools is not an effective development strategy because there is simply no investment return on education.
Population growth: In a country in which the majority of the population lives close to subsistence levels, an increase in income (e.g., by a technological improvement or by foreign aid inflows) primarily leads to a higher net rate of reproduction over the subsequent periods. The associated faster population growth puts additional strain on private and public investments, resulting in declines of physical and human capital whereby the economy remains trapped in the low-income equilibrium.
For an overview of different mechanisms that lead to the emergence of poverty traps see, for example, Galor and Weil (2000); Bloom et al. (2003a); Azariadis and Stachursky (2005); Galor (2005, 2011); Strulik et al. (2013); and Bloom et al. (2017).
Straightforward extensions of the baseline arguments of Solow (1956) and Diamond (1965) allow for a qualitative analysis of the dynamics of poverty traps. This analysis helps clarify why physical capital accumulation alone might not lift an economy out of poverty and why investments in human capital and fertility reduction are more promising. The canonical case of the dynamics of economic development in the presence of a poverty trap is shown in Figure 3. There are three intersections between the 𝐾t+1-curve and the 45° line such that three qualitatively different steady-state equilibria emerge. One steady-state equilibrium is at the origin, where the capital stock 𝐾′* is low and the economy is poor. Another equilibrium is at the capital stock 𝐾*, which corresponds to the prosperity equilibrium shown in Figure 2. In between these two equilibria, there is an unstable steady-state equilibrium, where the vertical red line intersects the 𝐾t+1-curve. If the economy starts with a capital stock that is lower than the capital stock corresponding to the level indicated by the vertical red line, the economy is caught in the basin of attraction of the poverty trap and converges to the low-income steady state (as indicated by the arrows in the diagram). Any policy that fails to raise the capital stock to a value above the vertical red line is insufficient to catalyze sustained growth.
Figure 3. Illustration of a possible poverty trap. If the initial stock of capital is located to the left of the vertical red line, the capital stock decreases over time and the economy shrinks towards the origin that represents the poverty trap.
Figure 4. Illustration of the effects of a policy that raises 𝐻̅ in case of the presence of a poverty trap. The 𝐾t+1-curve shifts upwards such that the basin of attraction of the poverty trap shrinks as compared to Figure 3.
There are two fundamentally different approaches to escaping such a poverty trap. The first is to invest massively in the accumulation of physical capital, whereby the economy ends up with a capital stock to the right of the vertical red line and in the basin of attraction of the high-income steady state. This “big push” strategy has been used as an argument in favor of immense foreign aid packages and expenditures on large infrastructure projects (cf. Murphy et al. 1989).
The second way to overcome the poverty trap is represented by policies targeted at increasing productivity 𝐴̅ and/or human capital 𝐻̅ to shift the 𝐾t+1-curve upwards. This shift leads to a shrinking basin of attraction of the poverty trap, as illustrated in Figure 4 in which 𝐻̅ increases to 𝐻̅′. Such an upward shift could be caused by investments in education, health, or fertility reduction. The next section discusses the particular pathways by which enhancing human capital may foster economic growth and reviews the empirical evidence in support of these mechanisms.
3. Literature Overview on the Qualitative and Quantitative Results of Different Investments
3.1. Pathways and Qualitative Findings
The following pathways have been suggested in the literature as explanations of the growth effects of education investments: better educated individuals (i) are more productive and, therefore, contribute more to aggregate output (Psacharopoulos, 1994; Hall and Jones, 1999; Bils and Klenow, 2000; Psacharopoulos and Patrinos, 2004, 2011); (ii) more readily embrace the adoption of productivity-enhancing technologies from abroad (Nelson and Phelps, 1966; Bloom et al., 2015); (iii) are more likely to establish successful and productive firms (Cabral and Mata, 2003; Bhattacharya et al., 2013; Gennaioli et al., 2013); and (iv) increase the productivity of their team members through spill-over effects (Lucas, 1988; Battu et al., 2003). Furthermore, a substantial body of macroeconomic literature finds education to be a key determinant of economic growth, suggesting that education’s impacts on individual productivity aggregate up to greater total productivity at the country level (see, for example, Barro 1991; Sala-i-Martin, 1997; Hanushek and Kinko, 2000; Krueger and Lindahl, 2001; Sala-i-Martin et al. 2004; de la Fuente and Domenech, 2006; Cohen and Soto, 2007; Hanushek and Woessmann 2012, 2015).
Similar pathways suggest that investments in health pay off over and above the increases in longevity and reductions in morbidity that are beneficial at the individual level. The following channels receive particular attention in the literature: (i) healthier workers are more productive and contribute more to aggregate output (Fogel, 1994, 1997; Shastry and Weil 2003; Weil, 2007; Bloom et al., 2018); (ii) healthier children tend to perform better in school, which enhances their potential for human capital accumulation (Miguel and Kremer, 2004; Bleakley and Lange, 2009; Field et al., 2009; Bleakley, 2010, 2011; Baldanzi et al., 2017; Bloom et al., 2017); (iii) healthier individuals are more inclined to educate themselves and to invest (Ben-Porath, 1967; Kalemli-Ozcan, 2000; Bloom et al., 2003c, 2007, 2014; Cervellati and Sunde, 2005, 2013; Prettner, 2013); and (iv) health investments that cure or prevent infectious diseases (such as vaccination) have positive spillovers to other individuals (Luca et al., 2018). Here, too, the positive effect found in micro-based studies is consistent with the macro-based evidence that health is an important determinant of economic growth (Barro 1991; Sala-i-Martin, 1997; Sala-i-Martin et al. 2004; Lorentzen et al., 2008; Suhrcke and Urban, 2010; Aghion et al., 2011; Cervellati and Sunde, 2011; Bloom et al., 2014; Bloom et al., 2018).
In addition to enhancing productivity, investments in education and health facilitate escape from fertility-induced poverty traps. Poor countries tend to have much higher youth dependency rates than wealthier countries. Supporting the basic needs of a relatively large child population imposes a substantial resource burden, necessitating the diversion of resources from other productive investments and ultimately impeding economic growth. While this high youth dependency partly reflects high infant and child mortality, it is primarily driven by the high fertility rates in these settings. As women become healthier, more educated, and more empowered, and as their expectations regarding child mortality improve, they tend to have fewer children, which helps to escape fertility-induced poverty traps and to converge onto a development path with low fertility and sustained economic growth (see Becker et al., 1990; Galor and Weil, 2000; Galor, 2005, 2011; Diebold and Perrin, 2013a, 2013b; Bloom et al. 2015; Prettner and Strulik, 2017 for the theoretical mechanisms and Brander and Dowrick, 1994; Ahituv, 2001; Li and Zhang, 2007; Herzer et al., 2012 for empirical evidence). The economic gains from lowering fertility (known as the “demographic dividend”) can be sizable (Bloom and Williamson, 1998; Bloom et al., 2003b, 2017; Golley and Tyers, 2015; Misra, 2015).
In addition, published research has revealed a second demographic dividend due to ageing (Mason and Lee, 2007), wherein persons expecting to live longer accumulate more assets in order to smooth consumption in old age.
3.2. Quantitative Results from the Literature
Quantitative assessments of the return on investment (ROI) in health, education, and fertility show that their impacts on productivity are sizeable. Psacharopoulos (1994), Hall and Jones (1999), Bils and Klenow (2000), and Montenegro and Patrinos (2014) demonstrate that, on average, income is 10% higher for each additional year of schooling. Psacharopoulos and Patrinos (2018) estimate even higher returns for low-income countries. In particular, average private rates of return to schooling are highest in Latin America and the Caribbean and for sub-Saharan Africa and lowest for Europe, the Middle East, and Northern Africa.
Table 2 illustrates the findings of four prominent studies regarding education and growth of per capita GDP. The relation between schooling and growth is positive and ranges from 0.2 to 12.5% per each additional year of schooling, with most of the estimates clustering in the range of 0.5% to 1.2%. A 25-point improvement in PISA score, a measure of educational quality, is similarly associated with a 0.5 percentage point (pp) increase in annual GDP per capita growth. These improvements in education may have a positive spillover effect on health as well (Pradhan et al., 2017, p. 424).
Table 2. Selected prominent studies on the relation between one-year increases in schooling and per capita GDP growth in percentage points
Sources
Relation with per capita GDP growth
Time frame
Coverage
de la Fuente and Domenech (2006, p. 28)
0.574 – 1.151% per schooling year
1960–1990
World
Cohen and Soto (2007)
1.05 – 1.26% per schooling year
1960–1990
World
Lutz et al. (2008, Fig. S1)
0.2 – 12.5% per schooling year
1970–2000
World
Hanushek and Woessmann (2012)
0.5% per 25 PISA test score points
1960–1990
World
The effects of health improvements on economic growth are quantified by Fogel (1997), Shastry and Weil (2003), and Weil (2007). Fogel (1997) provides historical evidence that improved nutrition (as observed over the period from 1780 to 1980 in Great Britain) raised the productivity of the workforce by 95%. Weil (2007) estimates that a 10% increase in the adult survival rate leads to a 6.7% increase in productivity per worker and a 4.4% increase in GDP per worker. The results of Shastry and Weil (2003) imply that differences in adult survival rates can explain even one third of cross-country variation in GDP per worker.
The macroeconomic estimates of Bloom et al. (2018) lie between the results derived by Shastry and Weil (2003) and Weil (2007) based on the aggregation of microeconomic effects. Bloom et al.’s results indicate that a 10% increase in the adult survival rate leads to a 9.1% higher productivity per worker. Measuring the causal impact of health on economic growth is a difficult task that requires tackling measurement and endogeneity issues. The results of selected studies that address these problems are included in Table 3.
Table 3. Selected prominent studies on the relation between increases in life expectancy and GDP per capita (or income) growth
Sources
Effect on growth
Time frame
Region
Bloom et al. (2014)
A 1-year increase in life expectancy raises per capita income between 5–15% over 60 years
1940–2000
World
Bloom et al. (2004)
A 1-year increase in life expectancy is associated with a 4% increase in long-run per capita output
1960–1990
World
Aghion et al. (2011)
A 1% increase in life expectancy is associated with 2.88–9.46% higher growth
1960–2000
OECD
Cervellati and Sunde (2011)
In post-demographic transition countries, a 1% increase in life expectancy is associated with a 1.94–4.14% higher growth rate
1940–2000
World
Bloom et al. (2018)
A 10% increase in adult survival rates is associated with a 9.1% increase in labor productivity
1960–2010
World
Weil (2007)
A 10% increase in adult survival rates increases labor productivity by 6.7% and GDP per worker by 4.4%
–
Australia, Denmark, Finland, France, Italy, Japan, Netherlands, Norway, Sweden, UK
Shastry and Weil (2003)
Changes in health can explain 19% of cross-country differences in per capita income
–
World
Ashraf et al. (2013) simulate output trajectories for different demographic scenarios and show that a reduction in the total fertility rate (TFR) of 0.5 children per woman raises per capita GDP by 11.9% after 50 years. Assuming linearity, this implies that a fall of the TFR by one child leads to an economic growth rate that is 0.45 pp higher (see also Bloom et al., 2017).
For Asian countries, the results of Bloom and Williamson (1998) and Bloom and Finlay (2009) suggest that one-third of East Asia’s “growth miracle” is due to the demographic dividend that followed the strong decline in fertility in these countries. This corresponds to an increase in GDP per capita growth by about 0.66% for each one-child reduction in the TFR. Even small changes in infant mortality—where lower fertility follows increased child survival—may substantially increase growth (see Table 4).
Table 4. Demographic dividends
Sources
Effects found
Time frame
Region
Bloom & Williamson (1998, p. 435-437)
A 1% higher growth rate of the working-age population is associated with 1.37–1.46% faster GDP per capita growth
1960–1990
East & Southeast Asia
Bloom & Finlay (2009, p. 58)
A 1% higher growth rate of the labor force is associated with 1.665% faster GDP per capita growth
1965–2005
World
We also analyzed literature studying the relationship between infrastructure spending and economic growth. Influential works (Barro, 1990; Canning & Pedroni, 2008) find that government—and especially infrastructure—spending may enhance development. Other findings (Crafts, 2009) suggest the effect is heterogeneous and sometimes offset by countereffects.
4. Empirical Analysis
The estimates presented in the previous section are drawn from a variety of sources that make use of different country samples, time frames, controls, and datasets (of varying quality). Furthermore, these studies utilize different econometric methods and take different types of costs and benefits into account. As such, these results are helpful for discerning the general impacts of different types of expenditures but do not lend themselves easily to straightforward comparisons of the relative ROI across sectors.
One main virtue of the original empirical analyses presented in this paper is that they estimate the impact of health, fertility, education, and infrastructure on GDP per capita simultaneously and under an internally consistent methodological framework. These analyses are able to better isolate the different relationships of interest and estimate their magnitudes in fully comparable manner. Our empirical strategy12 is based on growth regressions in both cross-country and panel data settings. Cross-sectional analyses are used to capture cumulative relationships over a relatively long time horizon. Here, we use initial levels of explanatory variables to explain economic growth over the following time period as a means of addressing issues of reverse causality. However, this does not control for confounding factors that may influence both initial levels of explanatory variables and subsequent growth, and thus does not fully address endogeneity concerns. As such, dynamic panel data methods are used to better infer causal impacts over a five-year interval.
The cross-country regressions explain annual per capita GDP growth rates between 1980 and 2015 as a function of initial income, share of equipment investments, initial levels of life expectancy, mean years of schooling, total fertility rate, electricity usage per capita (a proxy for infrastructure), share of the population of working age (15–64) to control for the initial demographic structure, and political rights (a proxy for institutions).13 In order to be consistent with the presence of poverty traps (described above), our data should exhibit multiple equilibria. As such, before proceeding to the formulation of the empirical strategy, we test the income data for the presence of multiple equilibria, or thresholds.
Three well-established modality tests are applied: the original Silverman (1981) test; the improved Hall and York (2001) test, specifically tuned for unimodality testing; and the Fisher and Marron (2001) test, which is superior in handling outliers. These tests reveal mixed evidence in favor of unimodality for GDP per capita analyses of 1960: the Hall and York (2001) test does not reject unimodality, whereas the Fisher and Marron test does. However, both tests reject unimodality in favor of bimodality for 1980 and 2015 numbers. From Figure 5, it follows that the 1980 modes are located near 8.02 and 10.2, corresponding to the low- and high-income equilibria, respectively. The antimode of 8.8 for 1980 serves as a virtual borderline between these two regimes. Notably, the threshold test for the multiple equilibria analysis points at 8.38, close to the antimode in 1980. For 2015, the modes are located near 8.21 and 10.71. This indicates that the income distribution has shifted higher but maintained bimodality, making the threshold analysis valid throughout the period.
Another important observation is the increase in dispersion among LMICs, reflecting the fact that countries like China, Indonesia, and South Korea moved to upper quartiles within the LMIC group, while other countries experienced very little growth. Strikingly, only South Korea managed the transition from the low-income equilibrium in 1980 to the high-income equilibrium in 2015. Understanding the modality and the implications of the presence of different income regimes is crucial for the estimation strategy, since the effects may have different magnitudes for different regimes (and may even offset each other).
12 An alternative strategy would be a micro-simulation using a general equilibrium model as in Kabajulizi et al. (2017) and Mohammed (2018), where the causal impact of expenditures is modeled for Uganda and Algeria, respectively. However, due to calibration issues, these simulations are generally better suited for specific countries rather than for large cross-country samples. Thus, we base our empirical approach on the well-established growth regression framework.
13 Political rights are included as a proxy for institutional quality because strong institutions facilitate better allocation of resources, more efficient investments, and more stable macroeconomic environments.
Table 5. Testing income modality
log GDP p.c.
Hall and York (2001) / Silverman (1981)
Fisher and Marron (2001)
H0: Unimodality
1960
0.08
0.044
1980
0.042
0.039
2015
0.043
0.028
H0: Bimodality
1980
0.96
0.662
2015
0.486
0.243
Note: for all tests 1000 bootstrapping rounds are conducted; support is derived from the range of the sample
13 More attention is due to nonlinearities in these relationships (e.g., diminishing returns to education) and interaction terms between variables (e.g., that investments in education may increase productivity to a greater extent when a population is healthy). However, inclusion of these extra terms did not improve the predictive power of the models developed in this paper, possibly due to the relatively small sample of countries.
Figure 5. Evolution of the log of GDP p.c. distribution from 1960 to 2015; same sample of 69
countries used for the estimation; critical bandwidths used from 1960, 1980 and 2015: 0.41,
0.26 and 0.4.
In order to address the problem of poverty traps, we apply single and multiple equilibria empirical strategy. The equation for the single equilibrium approach allows for one single set of coefficients:
The multiple equilibria approach, as in Hansen (2000), allows for multiple (two) sets of coefficients:
Here, 𝑦̂ is the annual growth rate of GDP per capita between time 𝑡₀ and 𝑇, 𝑦 is income at 𝑡₀, X is a matrix of growth determinants at 𝑡₀, 𝑢 is the error term, 𝑖 indicates country, and 𝛽 and 𝜃 represent the coefficients of interest, while 𝛾 and 𝑞 represent the threshold and threshold variable. We use initial levels of the selected growth determinants to limit the influence of endogeneity and reverse causality. For the threshold variable, we use log initial income to distinguish between low- and high-income equilibria.
In the single equilibrium estimations (Table 6, column 1), fertility was the most powerful predictor of growth. In this specification the only other significant effects were the convergence effects and the share of equipment investments. However, the single equilibrium approach may be problematic due to the fact that effects may vary in magnitude and sign across different segments of the data. The multiple equilibria analysis in Table 6 (columns 2 and 3) separately estimates effect magnitudes for low- and high-income countries (country list in Appendix A1). The threshold 𝛾 between low- and high-income countries is determined during estimation.14 This reflects persistent bimodality in income during the period of analysis.15 For countries in the low-income equilibrium, the following variables were significant: initial income, share of equipment investments, life expectancy, fertility, working-age population share, and rural population share. A 10% increase in life expectancy for low-income countries corresponds to a 0.39 pp increase in annual per capita GDP growth over the following 35 years. Increasing mean years of schooling by one year corresponds to a 0.27 pp increase in annual growth. Decreasing TFR by one child is associated with a 0.5 pp increase in growth for low-income countries and a 1 pp increase for high-income countries. No empirical evidence of heteroscedasticity was found and standard errors were used for both estimation strategies.
14 The multiple equilibria analysis assumes two regimes, consistent with the bimodal income distribution documented above.
15 Implementing these analyses with more than two regimes would be infeasible due to limited sample size.
Table 6. Single (1) and multiple equilibria (2 and 3) analysis; annual GDP p.c. growth rates during 1980–2015
Initial income is an intuitive variable for determining thresholds in the multiple equilibria analysis. However, other variables can be used to delineate thresholds as well: for example, Bloom and Canning (2007) focused on mortality traps and distinguish equilibria using life expectancy data. The state of the country with respect to the demographic transition can also be used to differentiate equilibria. Although correlated with income, the timing of a country’s demographic transition can provide additional perspective regarding variation in the determinants of economic growth among demographic transition forerunners, followers, trailers, and latecomers (Reher, 2004). Bimodality of fertility transitions is plausible and the Hall and York (2001) and Fisher and Marron (2001) tests both reject unimodality, with p-values of 0.022 and 0.0002, respectively. According to the threshold analysis, forerunners and followers belong to one regime, whereas trailers and latecomers belong to the other. Table 7 shows that using thresholds based on the timing of the demographic transition produces effect estimates that correspond reasonably well to those produced using initial income: for trailers and latecomers, life expectancy is significant and positive, and for forerunners and followers, mean years of schooling is the most significant determinant. Once again, fertility is significant and negative for both regimes, whereas life expectancy shows a negative effect for forerunners and followers.
Figure 6. Fertility transition years (Reher, 2004); sample of 58 countries; critical bandwidth: 10.35
Table 7. Multiple equilibria analysis; annual GDP p.c. growth rates during 1980–2015
To further minimize endogeneity bias and overcome other problems typical to cross-country growth regressions, we also construct a strongly balanced panel dataset encompassing 55 countries for the time span 1990–2015. In this estimation, we include the lag of GDP per capita to control for the convergence process and use five-year averages of the explanatory variables to smooth out business-cycle fluctuations, alleviate measurement errors, and focus on short-run effects. Panel data growth equations are estimated using the system generalized method of moments (SGMM) estimator (Blundell and Bond, 1998), treating all explanatory variables as endogenous. Explanatory variables are all lagged by one 5-year period and time fixed effects are included.
The dynamic threshold panel model from Dang et al. (2012) is used to apply the single and multiple equilibria approach for the panel data. This model is superior to non-dynamic threshold panel models, such as Hansen (1999), because it enables the usage of dynamic instruments for potentially endogenous regression, including the autoregressive term. The latter is a crucial control for the convergence effect. We use the same set of variables as in the cross-country regressions with the exception of fixed capital investments share, which is not available for the given time span and sample. Controlling for the lagged income should at least partly account for the stock of physical capital and therefore the absence of the latter control should not pose a major issue.
The dynamic threshold panel model from Dang et al. (2012) takes the following form:
where 𝑖 and 𝑡 are country and time indices with 5-year periods, 𝑦 is log GDP per capita, 𝑋 is a matrix of determinants and controls, 𝐼 is the indicator function for regime attribution, 𝑐 is the threshold (1 for low-income and 2 for high-income), 𝜌 and 𝜋 are coefficients, and 𝑣i,t is the composite error term.
In the single-equilibrium dynamic panel data estimation, fertility is the only significant predictor of economic growth: a one-unit decrease in TFR in the current 5-year period is associated with a 4.46% increase in GDP per capita in the next. Thus, the annualized effect of fertility is to increase per capita GDP growth by roughly 0.89 pp.
Under the multiple equilibria specification, the dynamic threshold panel model estimates significant effects for multiple variables: for the low-income equilibrium, the annualized effects of TFR, life expectancy, and schooling are all significant. A one-child decrease in the TFR is associated with a 2.1 pp increase in GDP per capita growth, an additional year of schooling with a 0.7 pp increase, and a ten percent increase in life expectancy with a 1.1 pp increase.
Notably, the threshold18 for this estimation lies close to 7.142, which is lower than in the cross-section threshold growth regressions and therefore can be interpreted as applying best to very low-income cases.19 In general, the short-run effects using the dynamic threshold panel model confirm the importance of health, education, and fertility in these settings.20
18 The Hansen (1999) model estimates similar values validating these results.
19 At least 12 countries from our sample would fall in this category at different time periods: Bangladesh, Benin, Cameroon, China, Congo (Dem. Rep.), Cote d’Ivoire, Ghana, India, Kenya, Myanmar, Nicaragua, and Nigeria. For the list of countries see Appendix, A2.
20 In addition, we conducted an impulse-response analysis [see Figure A8] using panel vector autoregressions to cross validate the effects in the short run using 3-year periods and explicitly address the impact of health and education expenditures on economic growth. The orthogonal cumulative impulse-response functions suggest that after 15 periods (45 years) the impact of health expenditures would prevail.
Table 8. Single (6) and multiple (7 and 8) equilibria SGMM estimation; 5-year log GDP p.c. levels, 1990–2015
To summarize, health and demography are again the most powerful predictors for economic growth and, thus, should be considered as priorities in policymaking. Schooling follows in terms of magnitude and robustness. Altogether, these results are consistent with the theoretical model suggesting that policies to reduce fertility, increase health, and bolster education are effective in helping an economy to escape from a poverty trap. The results are also consistent with the literature discussed in section 3.
5. Sub-sector Prioritization
The literature suggests that returns to education differ by education level and income setting. The Psacharopoulos and Patrinos (2018) meta-analysis shows that primary education is associated with a particularly high ROI in LMICs. The social return on investment in primary education is 22% in low- and 17% in middle-income countries, while the return on investment is substantially lower for secondary and tertiary education (see Table 9). This is consistent with the findings of Mingat and Tan (1996) and Petrakis and Stamatakis (2002), who show that low-income countries benefit most from investments in primary education. Investing in high-quality pre-primary education can also have huge positive returns, even in very low-income settings (Lomborg, 2018). Returns to girls’ education are generally higher than those for boys’ education and have important spillover effects through reducing TFR (Fink and Peet, 2016).
Table 9. Social returns to investments in education, 1960–2014
Low income
Middle income
Public
Primary
22.08%
17.10%
Secondary
18.10%
12.79%
Tertiary
13.18%
11.44%
Source: Meta-study of Psacharopoulos and Patrinos (2018)
In general, policies aimed at reducing gender inequality could be highly effective in boosting growth. Table 10 lists multiple studies suggesting that eliminating gender-based education gaps could yield approximately a 1% increase in economic growth. In addition, improvements in female education are associated with decreasing fertility, which has demonstrable effects on economic growth.
Table 10. Impacts of improving outcomes for women and girls
Source
Effects found
Time frame
Region
Bhalotra and Rawlings (2011)
Significant negative relationship between mothers’ health and neonatal/child mortality, low birthweight, and stunting
1970–2000
38 developing countries
Albanesi and Olivetti (2016)
Reductions in maternal mortality increased female labor participation and reduced disability years
1920–1990
US
Klasen (2018, pp. 292-294)
Eliminating gender gaps in education boosts growth by 0.8–1%
1960–2000
South & East Asia
Abu-Ghaida & Klasen (2004, p. 1082)
A one-year increase in female schooling reduces fertility by 8–13%
1975–2015
45 developing countries
Klasen (2004, p. 370)
Closing gender gaps would increase growth at least 0.9%
1960–1992
World
Altogether, particularly successful strategies for low-income countries would be targeted investments in women’s education—such as universal primary education for girls—and targeted interventions in women’s health, such as iodine supplementation and HPV vaccination. These female-focused interventions often create substantial knock-on effects by reducing fertility, which further accelerates economic growth.
The clearest and most comprehensive findings informing prioritization of health interventions come from the Copenhagen Consensus results, discussed in the next section.
6. Copenhagen Consensus Findings
The Copenhagen Consensus21 (CC) Center’s Post-2015 Consensus Project brought together economists and experts from the UN, NGOs, and the private sector to produce over 100 literature-informed reports on the effectiveness of the development targets proposed by the UN’s Open Working Group. The group of reports was reviewed by an expert panel that prioritized the interventions according to their value offered per dollar spent, including the value of discounted22 disability-adjusted life years. The aggregated research results of the Post-2015 Consensus priorities rank the returns to one US dollar spent from 2015 to 2030 on meeting these targets (Lomberg, 2018). The list of top-ranked interventions, provided in Table 11, highlights targets within general health, reproductive health, education, and other domains that merit particular focus.
It is worth noting that many of the CC’s recommended interventions have proven fairly stable over time: increasing availability of family planning, reducing under-nutrition among preschoolers, expanding access to tuberculosis treatment, promoting malaria prevention and treatment, and providing aspirin to reduce heart attack risk all ranked among the top 20 interventions in the previous two lists of CC recommendations released in 2008 and 2012.
Certain measures in the health sector can be listed as top priorities according to their returns: Nugent and Brouwer (2018) note that aspirin therapy at the onset of acute myocardial infarction can yield up to a 31-dollar return, mainly due to extremely low costs; reducing salt content in manufactured foods by at least 30% would yield 19 dollars; increasing tobacco prices by 125% through taxation would return around 10 dollars; chronic hypertension management for medium- to high-risk patients with at least 50% coverage could yield up to 7 dollars; and secondary prevention measures for cardiovascular diseases with at least 70% coverage could yield up to 3 dollars.
The above-mentioned returns concern noncommunicable diseases, yet communicable diseases are also considered a top priority: Raykar (2018) states that reducing malaria incidence by 50% could yield up to a 36-dollar return; Geldsetzer et al. (2018) report that increasing circumcision coverage to at least 90% of HIV-negative adult men would yield up to 28 dollars; and increasing antiretroviral therapy coverage to at least 90% of HIV-infected adults would yield around 10 dollars of return.
In addition, according to Kohler and Behrman (2018), universal access to sexual and reproductive health services and meeting the need for modern contraception could yield up to a 120-dollar return. With respect to overall returns to decreasing mortality, Jha et al. (2018) indicate that reducing premature mortality by 40% in low-income countries (LICs) could yield at least a 13-dollar return, whereas a decrease of the same magnitude in lower-middle-income countries (LMICs) would yield at least a 3-dollar return.
Prioritization of expenditures with respect to education is more complicated, yet a list of priorities from the Post-2015 Consensus can be derived as well: Psacharopoulos (2018) notes that an increase in preschool enrollment in sub-Saharan Africa from the present 18% to 59% could yield up to a 33-dollar return for each dollar spent, whereas increasing primary education enrollment from 75% to 100% could yield up to a 7-dollar return per dollar. The returns to other spheres of education are more volatile and involve higher uncertainty, though increasing completion rates at other levels of education (e.g., secondary) is also mentioned as a priority.
The above-mentioned priorities related to health and education should be considered in a broader context that also includes measures related to nutrition, food security, and corruption. The values in the table show that all these measures have very high returns above 100%.
21 The Copenhagen Consensus was established in Denmark in 2004 to respond to various global challenges and is now run by the U.S. non-profit Copenhagen Consensus Center. The 2015 conference focused on establishing sustainable development goals for the following 15 years.
22 In most studies, the discount rate of 3% was used.
Table 11. Top 10 post-2015 Consensus priorities
Category
Sub-category
Return to 1 USD
Reproductive health
Universal access to sexual and reproductive health (SRH)
120
Nutrition
Reduce by 40 per cent the number of children under 5 who are stunted
60
Illicit financial flows
Reduce to zero the legal persons and arrangements for which beneficial ownership info is not publicly available
49
Population and Demography
Reduce barriers to migration within low- and middle-income countries, as well as between low- and middle-income countries and high-income countries
45
Health
Reduce Tuberculosis deaths by 95% and TB incidence by 90%
43
Health
Delay artemisinin resistance greater than 1% and reduce malaria incidence using bed nets by 50%
36
Food security
Increase investment in agricultural R&D by 160%
34
Education
Increase the preschool enrollment ratio in sub-Saharan Africa from the present 18% to 59%
33
Health
Aspirin therapy at the onset of AMI (75% coverage)
31
Health
In hyper-endemic countries, attain circumcision coverage of at least 90% amongst HIV-negative adult men
28
7. Conclusions
During the last seventy years, many LMICs have experienced transformational economic growth while others experienced moderate to non-existent development gains. Governments of developing countries that have made substantial progress can take advantage of the resource expansion that came with their past growth experiences and invest in health, education, and infrastructure to promote further economic growth. Countries that have made only modest improvements can draw lessons from these disparate growth outcomes, in order to improve their growth trajectory going forward.
Using an intuitively accessible Solow model in discrete time, we show that i) investments in physical capital (e.g., infrastructure investments) could help a country escape a poverty trap and develop along a balanced growth trajectory only in the case of a “big push” scenario, while ii) investments in health and human capital would change the dynamic system and lift the balanced growth trajectory upwards, reducing the basin of attraction of the poverty trap, and making the transition to sustained growth easier.
We carry out our empirical analysis based on cross-sectional and dynamic panel data threshold regressions during the overall time frames from 1980 to 2015. Empirical analyses across multiple data sets, time frames, controls, and econometric estimators yields four main findings relevant to policymakers in LMIC settings:23
A one-child decrease in TFR corresponds to a 2 pp increase in annual GDP per capita growth in the short-run (5 years) and 0.5 pp higher annual growth in the mid- to long-run (35 years).
A ten percent increase in life expectancy at birth corresponds to a 1 pp increase in annual GDP per capita growth in the short-run and 0.4 pp higher growth in the mid- to long-run.
A one-year increase in average educational attainment corresponds to a 0.7 pp increase in annual growth in the short-run and 0.3 pp higher growth in the mid- to long-run.
Infrastructure proxies were not significantly associated with subsequent growth in any of the models estimated.
Given that per capita GDP growth in LMICs generally averages between 2% and 4%, the estimated changes in annual growth provided above are appreciable.24 The findings of these analyses are generally consistent with the theoretical and empirical literature.
23 The relationships between these variables likely vary with contextual factors. As such, the results presented should be understood as average, at-the-margin estimates. Additionally, as mentioned above and described in the manuscript, different methodologies are used to estimate short-run and mid- to long-run effects, so conclusions about the timeline of the return on benefits should be made cautiously.
24 In interpreting these results, it is important to consider the compounding effect of a persistent change in growth over several years. For example, a 1 pp increase in average annual economic growth from 3% to 4% cumulates to GDP per capita that is 3.9 times higher after a period of 35-years rather than 2.8 times higher.
Decisions on prioritizing governmental expenditures for economic growth should consider several factors alongside the average effects of the outcome variables on growth: the effectiveness of spending in improving the outcome variables, the timeline over which the effects of the spending will be realized, and validation using context-specific findings. Applying these metrics, reproductive health and fertility reduction tend to predominate as growth determinants. Policy measures related to this sector are most effective in the short- and medium-term time domains (5–15 years). Improving general health can be particularly effective in the medium term as well;25 however, most of the returns would be expected in the long run.
Education features a longer maturity horizon, although for low-income countries, some effects can be seen even in the middle term. Infrastructure projects have the broadest range in terms of findings and time domain. Our analyses suggest that this category showed less transformative potential than the others, but this does not suggest that a positive relationship between infrastructure spending and economic growth should be completely ruled out.
Priority setting within sectors is equally important: within health and education, investments in decreasing the burden of diseases, HIV and AIDS treatment and prevention, and preschool and primary education (especially for the low-income countries) show the most potential for growth. Growth spending priorities are not limited to these two sectors, as investments in improving gender equality can reduce fertility, increase the stock of human capital, and result in health improvements, all of which promote sustained economic growth.
It is important to consider that all of the results presented in this manuscript represent the average costs or benefits of different interventions and improvements in outcomes across countries, with the original empirical results excluding costs altogether. In reality, both the costs and benefits of achieving improvements in outcomes will vary substantially across settings and within the context of different programs. For example, a program to expand access to birth control may be highly successful in reducing fertility in a locality where unmet need for contraceptives is high, but completely ineffective in another environment where individuals desire a large number of offspring. As such, policymakers must consider the specific binding constraints to development in their settings, as well as the relative cost of the options available for achieving improvements in health, education, fertility, and infrastructure, in order to make sound assessments of their relative ROIs.
Ultimately, the decision over which interventions will best promote economic growth remains highly contextual, but well-informed decisionmakers should benchmark their expectations relative to the cross-country development experience of the last several decades.
25 See Table 8 for the panel data results and the related middle-term effects.
References
Abu-Ghaida, D. and Klasen, S. (2004). The Costs of Missing the Millennium Development Goal on Gender Equity. World Development 32(7), 1075-1107.
Aghion, P., Howitt, P., and Murtin, F. (2011). The relationship between health and growth: When Lucas meets Nelson-Phelps. Review of Economics and Institutions 2(1), 1-24.
Ahituv, A. (2001). Be fruitful or multiply: On the interplay between fertility and economic development. Journal of Population Economics 14(1), 51-71.
Albanesi, S. and Olivetti, C. (2016). Gender Roles and Medical Progress. Journal of Political Economy 124(3), 650-695.
Ashraf, Q., Weil, D., and Wilde, J. (2013). The Effect of Fertility Reduction on Economic Growth. Population and Development Review 39(1), 97-130.
Azariadis, C. and Stachursky, J. (2005). Poverty Traps. In P. Aghion & S. Durlauf (Eds.), Handbook of Economic Growth (Vol. 1A), 295-384, Amsterdam: Elsevier.
Baldanzi, A., Bucci, A., and Prettner, K. (2017). Children’s health, human capital accumulation, and R&D-based economic growth. Hohenheim Discussion Papers in Business, Economics and Social Sciences 01-2017, University of Hohenheim, Faculty of Business, Economics and Social Sciences.
Baldanzi, A., Prettner, K., Tscheuschner, P. (2019). Longevity-induced vertical innovation and the tradeoff between life and growth. Journal of Population Economics (forthcoming).
Barro, R. J. (1991). Economic growth in a cross section of countries. Quarterly Journal of Economics 106(2), 407-443.
Barro, R. J. (1990). Government Spending in a Simple Model of Endogenous Growth. Journal of Political Economy 98(5), 103-125.
Battu, H., Belfield, C. R., and Sloane, P. J. (2003). Human capital spillovers within the workplace: evidence for Great Britain. Oxford Bulletin of Economics and Statistics 65(5), 575-594.
Becker, G. S., Murphy, K. M., and Tamura, R. (1990). Human Capital, Fertility, and Economic Growth. Journal of Political Economy 98(5), 12-37.
Ben-Porath, Y. (1967). The production of human capital and the life cycle of earnings. Journal of Political Economy 75(4), 352-365.
Bhalotra, S. and Rawlings, S. (2011). Intergenerational persistence in health in developing countries: The penalty of gender inequality? Journal of Public Economics 95(3-4), 286-299.
Bils, M. and Klenow, P. J. (2000). Does Schooling Cause Growth? American Economic Review 90(5), 1160-1183.
Bleakley, H. (2010). Malaria eradication in the Americas: a retrospective analysis of childhood exposure. American Economic Journal: Applied Economics 2(2), 1-45.
Bleakley, H. (2011). Health, human capital, and development. Annual Review of Economics 2, 280-310.
Bleakley, H. and Lange, F. (2009). Chronic disease burden and the interaction of education, fertility, and growth. Review of Economics and Statistics 91(1), 52-65.
Bloom, D. E. and Williamson, J. G. (1998). Demographic transitions and economic miracles in emerging Asia (English). The World Bank Economic Review 12(3), 419-455.
Bloom, D., Canning, D., and Fink, G. (2014). Disease and Development Revisited. Journal of Political Economy 122(6), 1355-1366.
Bloom, D. E., Canning, D., and Graham, B. (2003c). Longevity and life-cycle savings. Scandinavian Journal of Economics 105(3), 319-338.
Bloom, D. E., Canning, D., Kotschy, R., Prettner, K., and Schünemann, J. (2018). Health and Economic Growth: Reconciling the Micro and Macro Evidence. IZA Discussion Paper No. 11940. IZA, Bonn, Germany.
Bloom, D. E., Canning, D., Mansfield, R. K., and Moore, M. (2007). Demographic change, social security systems, and savings. Journal of Monetary Economics 54(1), 92-114.
Bloom, D. E., Canning, D., and Moore, M. (2014). Optimal retirement with increasing longevity. Scandinavian Journal of Economics 116(3), 838-858.
Bloom, D. E., Canning, D., and Sevilla, J. P. (2003a). Geography and Poverty Traps. Journal of Economic Growth 8(4), 355-378.
Bloom, D. E., Canning, D., and Sevilla, J. P. (2003b). The demographic dividend. Population Matters. A RAND Program of Policy-Relevant Research Communication, Santa Monica, California.
Bloom, D., Canning, D., and Sevilla, J. (2004). The Effect of Health on Economic Growth: A Production Function Approach. World Development 32(1), 1-13.
Bloom, D. E. and Canning, D. (2007). Mortality traps and the dynamics of health transitions. Proceedings of the National Academy of Sciences of the United States of America 104, 16044-16049.
Bloom, D. E. and Finlay, J. (2009). Demographic change and economic growth in Asia. Asian Economic Policy Review 4(1), 45-64.
Bloom, D. E., Kuhn, M., and Prettner, K. (2015). The contribution of female health to economic development. NBER Working Paper 21411, National Bureau of Economic Research, Cambridge, Massachusetts.
Bloom, D. E., Kuhn, M., and Prettner, K. (2017). Africa’s prospects for enjoying a demographic dividend. Journal of Demographic Economics 83(1), 63-76.
Bloom, D. E., Kuhn, M., and Prettner, K. (2017b). Invest in Women and Prosper. Finance & Development 54(3), 50-55.
Bloom, D. E., Kuhn, M., and Prettner, K. (2018b). Escaping poverty: Investing in women’s human capital. In 2018 Davos Edition: Eradicating Extreme Poverty, Credit Suisse Research Institute, pp. 6-16.
Bloom, D. E. and Williamson, J. G. (1998). Demographic transitions and economic miracles in emerging Asia. World Bank Economic Review 12(3), 419-456.
Blundell, R. and Bond, S. (1998). Initial conditions and moment restrictions in dynamic panel data methods. Journal of Econometrics 87(1), 115-143.
Brander, J. A. and Dowrick, S. (1994). The role of fertility and population in economic growth: Empirical results from aggregate cross-national data. Journal of Population Economics 7(1), 1-25.
Burnside, C. and Dollar, D. (2000). Aid, Policies and Growth. American Economic Review 90(4), 847-868.
Cabral, M. B. L. and Mata, J. (2003). On the Evolution of the Firm Size Distribution: Facts and Theory. American Economic Review 93(4), 1075-1090.
Canning, D. and Pedroni, P. (2008). Infrastructure, long-run economic growth and causality tests for cointegrated panels. Manchester School 76(5), 504-527.
Cervellati, M. and Sunde, U. (2005). Human capital formation, life expectancy, and the process of development. American Economic Review 95(5), 1653-1672.
Cervellati, M. and Sunde, U. (2011). Life expectancy and economic growth: The role of the demographic transition. Journal of Economic Growth 16(2), 99-133.
Cervellati, M. and Sunde, U. (2013). Life expectancy, schooling, and lifetime labor supply: theory and evidence revisited. Econometrica 81(5), 2055-2086.
Cohen, D. and Soto, M. (2007). Growth and human capital: good data, good results. Journal of Economic Growth 12(1), 51-76.
Crafts, N. (2009). Transport infrastructure investment: implications for growth and productivity. Oxford Review of Economic Policy 25(3), 327-343.
Dang, V. A., Kim, M., and Shin, Y. (2012). Asymmetric capital structure adjustments: New evidence from dynamic panel threshold models. Journal of Empirical Finance 19(4), 465-482.
de la Fuente, A. and Domenech, R. (2006). Human capital in growth regressions: How much difference does data quality make? Journal of the European Economic Association 4(1), 1-36.
Diamond, P. A. (1965). National debt in a neoclassical growth model. American Economic Review 55(5), 1126-1150.
Durlauf, S. N., Johnson, P. A., and Temple, J. R. W. (2005). Growth Econometrics. In P. Aghion & S. Durlauf (Eds.), Handbook of Economic Growth (Vol. 1A), 555-677, Amsterdam: Elsevier.
Easterly, W., Levine, R., and Roodman, R. (2004). Aid, policies, and growth: Comment. American Economic Review 94(3), 774-780.
Fan, V. Y., Bloom, D. E., Ogbuoji, O., Prettner, K., and Yamey, G. (2018). Valuing health as development: going beyond gross domestic product. The BMJ 363:k4371.
Field, E., Robles, O., and Torero, M. (2009). Iodine deficiency and schooling attainment in Tanzania. American Economic Journal: Applied Economics 1(4), 140-169.
Fink, G. and Peet, E. (2016). Returns to Education in Low and Middle-Income Countries: Evidence from the Living Standards and Measurement Surveys. PGDA Working Paper 12014, Program on the Global Demography of Aging.
Fisher, N. I. and Marron, J. S. (2001). Mode testing via the excess mass estimate. Biometrika 88, 419-517.
Fogel, R. W. (1994). Economic growth, population theory, and physiology: the bearing of long-term processes on the making of economic policy. American Economic Review 84(3), 369-395.
Fogel, R. W. (1997). New Findings on Secular Trends in Nutrition and Mortality: Some Implications for Population Theory. In M. Rosenzweig and O. Stark (Eds.), Handbook of Population and Family Economics, Vol. 1A, 433-481, Amsterdam: Elsevier.
Galor, O. (2005). From Stagnation to Growth: Unified Growth Theory. In P. Aghion & S. Durlauf (Eds.), Handbook of Economic Growth (Vol. 1A), 171-293, Amsterdam: Elsevier.
Galor, O. (2011). Unified Growth Theory. Princeton, NJ: Princeton University Press.
Galor, O. and Weil, D. (2000). Population, technology, and growth: from Malthusian stagnation to the demographic transition and beyond. American Economic Review 90(4), 806-828.
Geldsetzer, P., Bloom, D., Humair, S., and Bärnighausen, T. (2018). Benefits and Costs of the HIV/AIDS Targets for the Post-2015 Development Agenda. In B. Lomborg (Ed.), Prioritizing Development: A Cost Benefit Analysis of the United Nations’ Sustainable Development Goals, 277-286. Cambridge: Cambridge University Press.
Gennaioli, N., La Porta, R., Lopez-de-Silanes, F., and Shleifer, A. (2013). Human capital and regional development. Quarterly Journal of Economics 128(1), 105-164.
Golley, J. and Tyers, R. (2012). Demographic Dividends, Dependencies, and Economic Growth in China and India. Asian Economic Papers 11(3), 1-26.
Hall, R. and Jones, C. (1999). Why do Some Countries Produce So Much More Output Per Worker than Others? Quarterly Journal of Economics 114(1), 83-116.
Hall, P. and York, M. (2001). On the calibration of Silverman’s test for multimodality. Statistica Sinica 11, 515-536.
Hansen, B. E. (1999). Threshold effects in non-dynamic panels: Estimation, testing, and inference. Journal of Econometrics 93(2), 345-368.
Hansen, B. E. (2000). Sample Splitting and Threshold Estimation. Econometrica 68(3), 575-604.
Hanushek, E. A. and Kimko, D. D. (2000). Schooling, Labor-Force Quality, and the Growth of Nations. American Economic Review 90(5), 1184-1208.
Hanushek, E. and Woessmann, L. (2012). Do better schools lead to more growth? Cognitive skills, economic outcomes, and causation. Journal of Economic Growth 17(4), 267-321.
Hanushek, E. and Woessmann, L. (2015). The Knowledge Capital of Nations: Education and the Economics of Growth. MIT Press, Cambridge, MA.
Herzer, D., Vollmer, S., and Strulik, H. (2012). The long-run determinants of fertility: One century of demographic change 1900-1999. Journal of Economic Growth 17(4), 357-385.
Jha, P., Hum, R., Gauvreau, C., and Jordan, K. (2018). Benefits and Costs of the Health Targets for the Post-2015 Development Agenda. In B. Lomborg (Ed.), Prioritizing Development: A Cost Benefit Analysis of the United Nations’ Sustainable Development Goals, 219-230. Cambridge: Cambridge University Press.
Kabajulizi, J., Keogh-Brown, M. R., and Smith, R. D. (2017). The welfare implications of public healthcare financing: a macro–micro simulation analysis of Uganda. Health Policy and Planning 32(10), 1437-1448.
Kalemli-Ozcan, S., Ryder, H. E., and Weil, D. N. (2000). Mortality decline, human capital investment, and economic growth. Journal of Development Economics 62(1), 1-23.
Klasen, S. (2002). Low Schooling for Girls, Slower Growth for All? Cross-Country Evidence on the Effect of Gender Inequality in Education on Economic Development. World Bank Economic Review 16(3), 345-373.
Klasen, S. (2018). The Impact of Gender Inequality on Economic Performance in Developing Countries. Annual Review of Resource Economics 10(1), 279-298.
Kohler, H. and Behrman, J. (2018). Benefits and Costs of the Population and Demography Targets for the Post-2015 Development Agenda. In B. Lomborg (Ed.), Prioritizing Development: A Cost Benefit Analysis of the United Nations’ Sustainable Development Goals, 375-398. Cambridge: Cambridge University Press.
Krueger, A. B. and Lindahl, M. (2001). Education for Growth: Why and for Whom? Journal of Economic Literature 39(4), 1101-1136.
Kuhn, M. and Prettner, K. (2016). Growth and welfare effects of health care in knowledge-based economies. Journal of Health Economics 46, 100-119.
Li, H. and Zhang, J. (2007). Do high birth rates hamper economic growth? Review of Economics and Statistics 89(1), 110-117.
Lomborg, B. (Ed.). (2018). Prioritizing Development: A Cost Benefit Analysis of the United Nations’ Sustainable Development Goals. Cambridge: Cambridge University Press.
Lorentzen, P., McMillan, J., and Wacziarg, R. (2008). Death and Development. Journal of Economic Growth 13(2), 81-124.
Luca, D. L., Iversen, J. H., Lubet, A. S., Mitgang, E., Onarheim, K. H., Prettner, K., and Bloom, D. E. (2018). Benefits and costs of the women’s health targets for the post-2015 development agenda. In B. Lomborg (Ed.), Prioritizing Development: A Cost Benefit Analysis of the United Nations’ Sustainable Development Goals, 244-254. Cambridge: Cambridge University Press.
Lucas, R. E. (1988). On the mechanics of economic development. Journal of Monetary Economics 22(1), 3-42.
Lutz, W., Crespo Cuaresma, J., and Sanderson, W. C. (2008). The demography of educational attainment and economic growth. Science 319(5866), 1047-1048.
Mason, A. and Lee, R. (2006). Reform and support systems for the elderly in developing countries: Capturing the second demographic dividend. Genus 62(2), 11-35.
Miguel, E. and Kremer, M. (2004). Worms: identifying impacts on education and health in the presence of treatment externalities. Econometrica 72(1), 159-217.
Mingat, A. and Tan, J. P. (1996). The full social returns to education: estimates based on countries’ economic growth performance. Human Capital Development and Operations Policy Working Paper HCD 73. Washington, DC: World Bank.
Misra, R. (2015). Impact of Demographic Dividend on Economic Growth: A Study of BRICS and the EU. International Studies 52(1-4), 99-117.
Mohammed, T. (2018). Simulation of the impact of economic policies on poverty and inequality: GEM in micro-simulation for the Algerian economy. International Review of Applied Economics 32(3), 308-330.
Montenegro, C. E. and Patrinos, H. A. (2014). Comparable estimates of returns to schooling around the world. Washington, DC: The World Bank.
Murphy, K. M., Shleifer, A., and Vishny, R. W. (1989). Industrialization and the Big Push. Journal of Political Economy 97(5), 1003-1026.
Nelson, R. and Phelps, E. (1966). Investment in humans, technological diffusion, and economic growth. American Economic Review 61(1-2), 69-75.
Nugent, R. and Brouwer, E. (2018). Benefits and Costs of the Noncommunicable Disease Targets for the Post-2015 Development Agenda. In B. Lomborg (Ed.), Prioritizing Development: A Cost Benefit Analysis of the United Nations’ Sustainable Development Goals, 231-243. Cambridge: Cambridge University Press.
Patrinos, H. A. and Psacharopoulos, G. (2011). Education: past, present and future global challenges. Policy Research Working Paper 5616. The World Bank, Washington, DC.
Petrakis, P. E. and Stamatakis, D. (2002). Growth and educational levels: a comparative analysis. Economics of Education Review 21(5), 513-521.
Pradhan, E., Suzuki, E. M., Martínez, S., Schäferhoff, M., and Jamison, D. T. (2017). The Effects of Education Quantity and Quality on Child and Adult Mortality: Their Magnitude and Their Value. In D. A. P. Bundy, N. de Silva, S. Horton, D. T. Jamison, and G. C. Patton (Eds.), Child and Adolescent Health and Development. Disease Control Priorities (third edition), Vol. 8, Ch. 30. Washington, DC: World Bank.
Prettner, K. (2013). Population aging and endogenous economic growth. Journal of Population Economics 26(2), 811-834.
Prettner, K. and Strulik, H. (2017). Gender Equity and the Escape from Poverty. Oxford Economic Papers 69(1), 55-74.
Pritchett, L. and Kenny, C. (2013). Promoting millennium development ideals: the risks of defining development down. CID Working Paper 265. Harvard University, Center for International Development, Cambridge, MA.
Psacharopoulos, G. (1994). Returns to investment in education: A global update. World Development 22(9), 1325-1343.
Psacharopoulos, G. and Patrinos, H. A. (2004). Returns to investment in education: a further update. Education Economics 12(2), 111-134.
Psacharopoulos, G. and Patrinos, H. A. (2018). Returns to investment in education: a decennial review of the global literature. Education Economics 26(5), 445-458.
Psacharopoulos, G. (2018). Benefits and Costs of the Education Targets for the Post-2015 Development Agenda. In B. Lomborg (Ed.), Prioritizing Development: A Cost Benefit Analysis of the United Nations’ Sustainable Development Goals, 119-142. Cambridge: Cambridge University Press.
Raykar, N. (2018). Benefits and Costs of the Malaria Targets for the Post-2015 Consensus Project. In B. Lomborg (Ed.), Prioritizing Development: A Cost Benefit Analysis of the United Nations’ Sustainable Development Goals, 287-294. Cambridge: Cambridge University Press.
Romer, P. (1990). Endogenous technological change. Journal of Political Economy 98(5), 71-102.
Reher, D. S. (2004). The Demographic Transition Revisited as a Global Process. Population, Space and Place 10, 19-41.
Sachs, J. D. (2005). The End of Poverty: Economic Possibilities for Our Time. New York: The Penguin Press.
Sala-i-Martin, X. (1997). I Just Ran Two Million Regressions. American Economic Review 87(2), 178-183.
Sala-i-Martin, X., Doppelhofer, G., and Miller, R. I. (2004). Determinants of Long-Term Growth: A Bayesian Averaging of Classical Estimates (BACE) Approach. American Economic Review 94(4), 813-835.
Shastry, G. and Weil, D. (2003). How Much of Cross-Country Income Variation Is Explained by Health? Journal of the European Economic Association 1(2-3), 387-396.
Silverman, B. W. (1981). Using kernel density estimates to investigate multimodality. Journal of the Royal Statistical Society: Series B 43, 97-99.
Solow, R. M. (1956). A contribution to the theory of economic growth. Quarterly Journal of Economics 70, 65-94.
Strulik, H., Prettner, K., and Prskawetz, A. (2013). The past and future of knowledge-based growth. Journal of Economic Growth 18(4), 411-437.
Suhrcke, M. and Urban, D. (2010). Are cardiovascular diseases bad for economic growth? Health Economics 19(12), 1478-1496.
Weil, D. N. (2007). Accounting for the effect of health on economic growth. Quarterly Journal of Economics 122(3), 1265-1306.
Appendix
A1. List of countries for Table 5
Cross-section
Low-income equilibria
High-income equilibria
Algeria
Bangladesh
Benin
Bolivia
Cameroon
Colombia
Congo, Rep.
Cote d’Ivoire
Dominican Republic
Ecuador
El Salvador
Ghana
Guatemala
Honduras
India
Jamaica
Jordan
Kenya
Korea, Rep.
Malaysia
Mauritius
Morocco
Mozambique
Nepal
Nicaragua
Pakistan
Paraguay
Peru
Philippines
Senegal
Sri Lanka
Thailand
Tunisia
Zambia
Zimbabwe
Argentina
Australia
Austria
Belgium
Brazil
Canada
Chile
Costa Rica
Cyprus
Denmark
Finland
France
Germany
Greece
Hong Kong
Ireland
Israel
Italy
Japan
Mexico
Netherlands
Norway
Panama
Portugal
Singapore
Spain
Sweden
Switzerland
Trinidad and Tobago
Turkey
United Kingdom
United States
Uruguay
Venezuela
A2. List of countries for Table 7
Panel data
Low-income equilibria
High-income equilibria
Bangladesh
Benin
Cameroon
China
Congo (Dem. Rep.)
Cote d’Ivoire
Ghana
India
Kenya
Myanmar
Nicaragua
Nigeria
Algeria
Argentina
Australia
Austria
Belgium
Bolivia
Brazil
Canada
Chile
Colombia
Congo, Rep.
Costa Rica
Cuba
Cyprus
Denmark
Dominican Republic
Ecuador
Egypt
El Salvador
Finland
France
Gabon
Germany
Guatemala
Honduras
Hong Kong
Iceland
Indonesia
Iraq
Ireland
Israel
Italy
Jamaica
Japan
Jordan
Korea, Rep.
Luxembourg
Malaysia
Malta
Mexico
Morocco
Netherlands
New Zealand
Table A3. Descriptive statistics for expenditure levels by quartiles of initial income
Levels of expenditures
Variable
Average, %
Coefficient of variation, %
A. First quartile based on initial income
GDP p.c. growth rates
4.595
0.4488
Health expenditures
10.013
0.2861
Education expenditures
3.794
0.3206
Infrastructure expenditures
0.860
1.8053
B. Second quartile based on initial income
GDP p.c. growth rates
3.351
0.2965
Health expenditures
11.712
0.2818
Education expenditures
4.254
0.1842
Infrastructure expenditures
0.464
0.5925
C. Third quartile based on initial income
GDP p.c. growth rates
1.767
0.4095
Health expenditures
13.930
0.1727
Education expenditures
5.045
0.1837
Infrastructure expenditures
0.665
0.5416
D. Fourth quartile based on initial income
GDP p.c. growth rates
1.414
0.2859
Health expenditures
14.027
0.1430
Education expenditures
5.411
0.2529
Infrastructure expenditures
0.756
0.5136
Note: initial income is measured in 1995 in logarithms; GDP p.c. growth rates are measured during 2005–2015; expenditure levels are measured as share of GDP in 1995–2005.
Table A4. Descriptive statistics for expenditure growth rates by quartiles of initial income
Growth rates of expenditures
Variable
Average, %
Coefficient of variation, %
A. First quartile based on initial income
GDP p.c. growth rates
4.595
0.4488
Health expenditures
9.450
0.7100
Education expenditures
7.187
0.6691
Infrastructure expenditures
29.582
1.1028
B. Second quartile based on initial income
GDP p.c. growth rates
3.351
0.2965
Health expenditures
5.362
0.5202
Education expenditures
4.522
0.4745
Infrastructure expenditures
30.800
1.0902
C. Third quartile based on initial income
GDP p.c. growth rates
1.767
0.4095
Health expenditures
2.900
0.3624
Education expenditures
2.671
0.8032
Infrastructure expenditures
22.825
1.6432
D. Fourth quartile based on initial income
GDP p.c. growth rates
1.414
0.2859
Health expenditures
2.319
0.4375
Education expenditures
2.779
0.7172
Infrastructure expenditures
10.142
0.6191
Note: initial income is measured in 1995 in logarithms; GDP p.c. growth rates are measured during 2005–2015; expenditure growth rates are measured in 1995–2005.
Figure A5. Health Expenditures vs. per capita GDP Growth (outliers removed)
Figure A6. Education Expenditures vs. per capita GDP Growth (outliers removed)
Figure A7. Infrastructural Expenditures vs. per capita GDP Growth (outliers removed)
Figure A8. Panel VAR cumulative impulse-response functions for health and education expenditures using 3-year periods
David E. Blooma, Alexander Khourya, Vadim Kufenkob, and Klaus Prettner
High-quality delivery systems are effective at achieving outcomes, efficient at utilizing resources, equitable at providing services, and resilient in the face of challenges.
A high-quality health system should support the physical, mental, and social wellbeing of the people it serves and a high-quality education system should help students reach their full potential as productive members of society. The likelihood of achieving improvements in the health, education, and economic development of a population hinges on the quality of the underlying and interrelated health and education delivery systems.
This policy brief provides an overview of three key areas in health and education: human resource motivation and performance; procurement, supply delivery and management; and data for decision-making. It reviews challenges and potential policy options to guide quality improvement efforts in those areas. A summary table is included in Annex 1.
Human resource motivation and performance are fundamental to equitable service provision and effective achievement of health and education outcomes. Key challenges include absenteeism; professional attrition (either to urban areas or high-income countries); and low technical competence. Root causes of these challenges include inadequate professional training; stressful working conditions; scarcity of essential supplies and materials; heavy and increasing workloads; low and unreliable remuneration; and lack of opportunities for growth and professional development.
Policy options to tackle these challenges could include reforming remuneration schemes to create a stronger link between payment and performance indicators. Changes could also be made to the recruitment and deployment strategies for health and education workforces, including setting higher admissions standards into the profession, diversifying the workforce and putting in place measures to attract and retain staff in underserved areas. Policies could also include enhanced professional development programs, either in-service or using technology to facilitate remote learning and supervision. Finally, technology could also be integrated into monitoring and service delivery systems to make them more accountable and responsive.
Procurement, supply delivery, and management systems critically affect efficient resource utilization and effective achievement of health and education outcomes. In education, the provision of textbooks is a challenging area for supply chain and procurement, but one which yields excellent returns on investment. Across both the health and education sectors, weaknesses in national procurement and supply chain systems are leading to stockouts and waste of essential supplies, inflated prices, and poor quality of products (including counterfeit or ineffective medicines). The causes of these issues range from high production and import costs, difficulties with making accurate forecasting and requisition estimates, inadequate storage and transportation conditions (which can lead to theft or damage), as well as diffused responsibility in the underlying accountability structure and unpredictable financing.
Effective policies to strengthen these systems should be carefully adapted to the local context and capacity but could include seeking procurement agreements with national or regional producers, the private sector, or through a pooled funding arrangement. Policies could also aim to centralize procurement or streamline the distribution of essential goods, while also potentially reducing the number of wholesalers and intermediaries to drive down costs. Distribution processes could be improved through investments in strengthening the stock-management and requisition systems at local levels (potentially enabled by technology), shortening the lag between replenishment cycles, and integrating systems for improved product traceability and efficient transportation. Finally, focusing on developing and retaining a qualified procurement and supply chain workforce is an important area to consider.
Data-driven decision making is a fundamental delivery tool that impacts the equity, efficiency, resilience, and effectiveness of a delivery system. The availability of quality data is often inadequate in many low- and middle-income countries (LMICs) as well as underutilized when available. Data from health and education systems are often managed in a fragmented system with little capacity for rapid and digestible analysis and dissemination. At the root of this situation is a history of underfunding national statistics offices, an over-emphasis on donor-driven aggregated surveys for cross-national comparisons over disaggregated and actionable national-level data, as well as weak demand for data from users (from government decision makers to citizens).
To enact the “data revolution” called for by the UN, initiatives should be put into place to improve the quality of data, through financing more robust national statistical offices, performing enhanced data audits and better aligning donor and local data streams. The key indicators for each sector should be chosen to reflect the desired outcomes (quality) and not just quantity and should include regularly administered internationally recognized standard measures. Policies should also be enacted to create a culture of “demand for data” at every level, as well as working with data producers to create user-friendly products that meet the needs and are easily actionable for decision makers.
Introduction
There has been increased attention in recent years on moving beyond accessing services to focusing on the quality of service delivery across health and education. High-quality delivery systems are effective at achieving outcomes, efficient at utilizing resources, equitable at providing services, and resilient in the face of challenges. Thus, a high-quality health system should support physical, mental, and social wellbeing of the people it serves and a high-quality education system should help students reach their full potential as productive members of society. The likelihood of achieving improvements in the health, education, and economic development of a population hinges on the quality of the underlying and interrelated health and education delivery systems.
Strategies to improve quality must include policies to improve resource utilization and service delivery in three key areas: human resource motivation and performance; procurement, supply delivery and management; and data for decision-making. This brief will seek to provide context, as well as possible policy options and combinations, to guide quality improvement efforts.
Quality in health systems
A recent Lancet Global Health Commission on High Quality Health Systems in the SDG Era1 has called for “a revolution” in health care quality. Despite gains in health outcomes globally, the commission points to the often poor quality of care provided across LMIC, which leads to nearly eight million avoidable deaths each year. As countries strive to provide universal health coverage (UHC), an integral part of achieving SDG 3 “Good health and well-being,”2 they must also make improving quality a core component of these efforts, together with expanded coverage and financial protection. The Commission’s report includes among the foundational elements of high-quality health systems: workforce numbers and skills, tools and resources from drugs to data, as well as the capacity to analyze and learn from data.1
Quality in education
Since 2000, there has been enormous progress around the world toward achieving Millennium Development Goal (MDG) 2: universal primary education. Total enrollment rates reached 91% in 2015 in developing regions, and the number of children out of school was halved.3 However, these efforts have often eclipsed concerns around the quality of education, a concept which encompasses the learners’ cognitive development and the “promotion of values and attitudes of responsible citizenship and in nurturing creative and emotional development.”4 The 2018 World Development Report has called the current situation a “learning crisis,” with hundreds of millions of children worldwide failing to learn basic arithmetic and reading skills. To address this, SDG 4 is concerned explicitly with “quality education.”
Within UNESCO’s framework for understanding education quality,4 “enabling inputs for quality education” include teaching and learning materials, physical infrastructure and facilities, human resources (teachers, principals, inspectors, supervisors, and administrators), as well as school governance.
Human Resource Motivation and Performance Overview
Worker performance is highly linked to worker motivation due to the labor-intensive and interpersonal nature of the services being provided. The performance of health professionals (though relevant to education professionals as well) has been defined as being available – retained and present – competent, productive, and responsive.5 A WHO framework for health worker performance and its link to motivation is in Annex 2.
Motivation has been defined as “an individual’s degree of willingness to exert and maintain an effort towards organizational goals.”6 This definition also frames motivation as being composed of two components: “the extent to which workers adopt organizational goals (‘will do’) and the extent to which workers effectively mobilize their personal resources to achieve joint goals (‘can do’).”
Herzberg7 provides a theoretical foundation for the determinants of motivation that is grounded in two types of factors:
Dissatisfaction avoidance or hygiene factors
Growth or motivator factors
Organizational policy and administration
Supervision
Interpersonal relationships
Salary
Status
Job security
Working conditions
The work itself
Achievement
Recognition
Responsibility
Growth or advancement
While financial incentive levels and schemes may be important determinants of worker motivation, they alone have been found to be insufficient to keep health professionals motivated. A motivated worker must also have the right competencies, work environment, and resources to be high performing.5
Challenges in Human Resource Motivation and Performance
The challenges relating to human resource motivation and performance in health and education systems are considerable.
Absenteeism: Many countries have epidemic levels of teacher and health worker absenteeism, particularly in rural and remote areas. A study in six developing countries found an average of 19% of teachers and 35% of health workers were absent during regular working hours.8 In India, more than 23% of teachers were absent during unannounced school visits, which was associated with an annual cost of $1.5 billion for services that were not delivered.9
Professional attrition and “brain drain”: Teacher attrition rates in sub-Saharan Africa are variable but high—between 5-30%,10 and yet demand for teachers in low-resource countries is expected to grow dramatically in the years ahead, nearly doubling by 2030.11 Similarly, for health professionals in LMICs, migration to urban areas or higher-resource countries is mostly unplanned, leading to a “brain drain” of talented professionals and exacerbating shortages in resources in health. Despite efforts by the WHO to curb this trend, physician density is still declining in the majority of African countries and physician migration is on the rise.12
Low technical competences in teaching and care: A study of nine sub-Saharan African countries using Service Delivery Indicators (SDI) found very weak rates of adherence to clinical guidelines. Less than a third of providers adhered to guidelines for neonatal and maternal health complications, and 35.9% adhered to guidelines for diarrhea, pneumonia, and malaria, with a diagnostic accuracy for these conditions of only 50%. Similarly poor guideline adherence was found in studies in health centers in India.13 Concerns also exist with the quality of teaching. The Learning Barometer survey of student performance, carried out in 28 African countries with primary school-age learners (Grades 4 and 5), identifies the proportion of children who meet a minimum learning threshold. It found that over a third of students—23 million children—fell below the minimum learning threshold, meaning most will be “unable to read or write with any fluency, or to successfully complete basic numeracy tasks.”14
Root Causes of These Challenges
Several of the root causes of the aforementioned challenges are described below.
Inadequate initial professional training: Many teachers graduate from their training lacking information on what their pupils are supposed to learn and basic teaching and curricular management skills.14 Training programs for health care professions also suffer from chronic under-investment.15 A survey of medical schools across Africa found “ubiquitous faculty shortages in basic and clinical sciences, weak physical infrastructure, and little use of external accreditation.”16
Difficult working conditions, including insufficient physical and supportive infrastructure: Schools and health centers, particularly in rural areas, can lack the very basics such as running water, consistent electricity, and adequate sanitation facilities.17,18 Access to decent housing and family-centered services (schools, daycare) outside of urban areas is also a major challenge for many professionals in education19 and health,20 particularly for women.
Lack of work materials and essential supplies: (discussed in the following section)
Increasing workloads: Pupil to Teacher Ratios (PTR) have increased dramatically following the roll-out of Universal Primary Education policies. This has meant overcrowded classrooms, more teaching periods, and more non-teaching activities.17 The global needs-based shortage of health-care workers is projected to be 14 million by 2010. When taking into account population size, the most severe challenges are in sub-Saharan Africa, where ratios of health professionals to patients are predicted to worsen between 2013 and 2030.15
Low and unreliable remuneration: In many countries, teachers and health care providers do not earn enough to live above the poverty line, requiring many to turn to other part-time work to supplement their income.5,19 They may also experience delays in receiving their salary and be required to travel long distances to receive it.17
Lack of constructive supervision, professional recognition or professional development opportunities: Education systems in many countries report having infrequent or ineffective supervisory visits. Teachers also generally receive very little feedback, support, or advice from more senior teachers or school administrators on how to improve.14 Similarly, health professionals have often limited access to professional development opportunities, which tend to be unevenly distributed despite high demand.17
Policy Options to Improve the Motivation and Performance of Human Resources
Below is an overview of policy options that could be considered to improve the motivation and performance of health and education professionals.
It must be noted that worker motivation is sensitive to system-wide or facility reform processes which can affect organizational dynamics, reporting, accountability and incentive structures. These changes may elicit a range of responses from professionals as they often require the development of new workforce capabilities and can affect different health system cadres differently.6 The involvement of health workers in the design and implementation of reforms has been found to be an effective way to manage these concerns.5
Policies to improve motivation and performance can be undertaken at the macro-system level or at the micro-facility level and can be designed to address performance issues by tackling “can do” or the “will do” gaps. They can also address the living conditions of health workers in ways that are adapted to the context, including rural location, age and gender considerations.5
Option 1. Changes to Payment and Reward Systems
Creating stronger linkages between payment and performance indicators can be an important way to improve the quality of professional work. The implementation of reforms to payment schemes requires careful consideration of bureaucratic and political economy considerations, such as resistance from unions, and the required data collection infrastructure.21
Health worker performance-based financing (PBF or P4P) schemes: PBF is a contracting mechanism designed to increase the performance and quality of service providers by offering financial incentives to health facilities for the provision of a defined set of services, with adjustments based on measures of quality. These vary considerably in their format (payment structure, target services, etc.) and effect on employee performance and health outcomes.22 In the past decades, PBF schemes have generated substantial interest among policy-makers, donors and international organizations; as of 2015 a dedicated trust fund at the World Bank alone supported 36 PBF programs.23 Conditional cash transfers, modified by quality measurements, were found to be particularly effective in Rwanda – where P4P was found to have a positive effect on health care utilization, quality of care and outcomes, as well as on lowering worker absenteeism.24-27
Teacher performance pay schemes: Numerous schemes exist to reward teachers based on specific measures of performance and outputs. Studies in Tanzania, India and China generally found these approaches to be effective when combined with providing resources such as unconditional grants or textbooks.25,28,29 However, several other evaluations showed either no or marginally positive gains from such measures, especially for low-performing schools. It was also found that rewards may have detrimental effects, such as diminishing peer collaboration, narrowing the curriculum, and over-emphasis of teaching to the test. Generally, these schemes remain relatively rare at scale – a review found that only 17 of 101 education systems used test scores to formally sanction or reward schools or educators.30
Benchmarking: Payments are based on the number of students that reach specific proficiency levels. This was found to be easier to communicate and implement,31 but difficult to sustain.32
Pay for Percentile: Payments are based on students’ test scores relative to other students at the same starting level or similar students in other schools. This is harder to implement but incentivizes teachers to improve learning across the entire student distribution.33
Special awards for teaching quality: Particularly when recognizing collaborative work among teachers, as research has found that monetary incentives are more effective when awarded to teaching teams compared to individual teachers.34
Option 2. Changes to Recruitment and Deployment
Macro-level policies can aim to improve education and health workforces by targeting who is recruited into key professions, how they are trained, and where they are deployed to work.
Higher standards for recruitment: Setting higher minimum qualifications to enter the teaching or nursing profession, such as an undergraduate degree, could be an effective way to improve the status of the profession as well as to attract high-performing individuals. A merit-based appointment system, such as one implemented in Pakistan for teacher recruitment, included a test administered by a third-party National Testing Service to protect the system from political influence.35
Measures to attract and retain professionals in understaffed rural areas: Several initiatives have been found to be effective for health care workers, including providing preferential admissions to students from rural areas, designing a “rurally oriented curricula” with a focus on rural health issues, imposing compulsory training rotations in rural settings, as well as providing scholarships, financial incentives, professional advancement, support networks, and help with setting up medical practices in rural areas.20 In education, other non-monetary incentives have been used, such as offering bicycles, housing, and preferential access to resources and training. “In the short term, the provision of good quality housing with running water and electricity for teachers is probably the most cost-effective way of attracting and retaining teachers at hard-to-staff rural schools.”19
Diversification of the health and education workforce: To minimize the time spent by teachers on non-teaching activities, it is possible to include pedagogic assistants, health practitioners, and administrative support.11 Similarly in health care, shifting tasks between health care workers (“task sharing”) and expanding the clinical team, particularly to include community health workers, can relieve short-term human resource limitations.18
Option 3. Enhanced Professional Development Programs
Opportunities to improve existing or develop new technical skills are often a major source of motivation for professionals in health and education, and they also directly address the “can do” gap that inhibits performance.
In-service or facility-based skills-development programs: Training is best when done close to practice where learners can immediately apply concepts and receive feedback. Meta-analyses show that successful in-service teacher training, coupled with ongoing monitoring, mentoring, and coaching, is a proven way to improve primary school teachers’ instructional practice in LMICs.36,37 Such approaches are generally more expensive but preferable to external continuing education programs or training-of-trainers cascade models, which have the disadvantage of being expended on a small minority of professionals who are withdrawn from their work.38
Training and skills-building programs specific to management professionals: In addition to frontline workers, initiatives to develop the skills of managers are an important part of improving overall system quality. Health facility management training and supervision were found to be effective at improving organizational practices and health outcomes but needed to be ongoing.39 Training programs for headmasters in school management and leadership were also found to be effective across 13 countries at improving teacher motivation and performance.19,34
Technology-enabled training and support: Some initiatives, such as technology-assisted professional development and text-message support, have been used to effectively reach teachers in remote areas.40,41
Option 4. Integration of Technology into the Classroom or the Clinic
Technological innovations, from apps to integrated teaching and learning systems, are multiplying in health and education spaces. These present great opportunities for improved performance, but also require significant investments and infrastructure. Across many developing countries, the rate of internet connectivity in schools is less than 10%. There is some concern that uneven access to these resources could exacerbate existing learning inequalities between rural/urban or affluent/resource-constrained areas.11 Nevertheless, technological innovations have been deployed to achieve a number of goals.
“Blended-learning classrooms”: This format combines learning using technology with face-to-face teaching and was found to be effective in several case studies.41
Technology for improved attendance monitoring: Different approaches have been tried to reduce absenteeism, including using sophisticated surveillance technology or simple mobile phone text systems. Biometric attendance monitors in primary health centers or cameras in schools in India were only found to be effective when attendance was linked to rewards or penalties and there was sufficient buy-in from the stakeholders involved in these processes.42 Other simple phone-based platforms to send daily data on teacher attendance were found to be effective in the Gambia and Zimbabwe.43
Procurement, Supply Delivery and Management Overview
Functioning procurement, supply delivery, and management systems are essential for quality health and education service delivery. A supply chain encompasses an “ecosystem of interlinked organizations, people, technology, activities, information, and resources” that is required to get products from manufacturers to users in the most cost-effective way possible. This includes inventory management, storage, distribution, and inventory control, and requires a large, competent, and properly trained workforce. Supply chains do more than simply delivering products, they also produce critical information related to the need, demand, and consumption to national and regional level planners.44
Procurement and Supply Chains in Health
The structure of supply chains for health varies greatly depending on national health system characteristics, such as the different sources of financing, risk pooling and purchasing, as well as national pharmaceutical regulations and treatment-seeking behaviors of patients. Supply chains play a role in many dimensions of health system performance: payment, organization, regulation, and also behavioral aspects of the health system.44 In the coming decades, as many global health initiatives such as GAVI, the Global Fund, and PEPFAR roll back their support, many LMICs will need to play a larger role in the procurement of health products.45
Procurement and Supply Chains in Education
Access to appropriate learning materials is listed as a key strategy for achieving SDG4 – particularly the dimension related to providing inclusive and effective learning environments for all.3 Textbooks are a particularly important input for improving learning outcomes in contexts with large class sizes, under-qualified teachers, and shortened instructional time. They have been found to be, when they are in the appropriate language and level of difficulty, a particularly cost-effective input with high returns in student achievement.30 A multi-country study of 22 sub-Saharan African countries found that providing one textbook to every student in a classroom increased literacy scores by 5–20%.46
Challenges in Procurement, Supply Delivery and Management
Supply chains can significantly affect the availability, price, and quality of strategic inputs. However, many national procurement and supply chain systems remain ineffective and poorly managed.
Lack of availability of working materials and supplies: Key health system inputs, such as medicines, are not consistently available in many low-resource settings. According to an analysis of WHO data, the average availability of generic medicines in the public sector ranges between 29% to 54% across WHO regions.47 Interruptions in the access of medications are an important threat to public health, as they interfere with treatment initiation or continuity and increase the likelihood of ill health and antimicrobial resistance.45 Similarly, the procurement and supply of essential learning materials, particularly quality textbooks, remains a challenge in many LMICs. Between 2000 and 2007, rapid enrollment increases were experienced across several LMICs; however, textbook availability could not keep up. For example, in Malawi, “the percentage of students who either had no textbook or had to share with at least two other pupils increased from 28% in 2000 to 63% in 2007.”46 Gaps in essential school supplies are even more pronounced in rural or underserved areas.
Inflated prices: Across LMICs, the prices of many vital inputs for health and education systems can be variable and disproportionately high. According to an analysis of WHO data, median government procurement prices for 15 generic medicines are 1-11 times international reference prices, and procurement prices that were low did not always translate to lower patient prices. This created a situation in which “treatments for acute and chronic illness were largely unaffordable in many countries.”47 The cost of textbooks varies greatly by country and region. In sub-Saharan Africa, the unit cost of a primary school textbook is between US$2 and US$4 compared to Vietnam, which produces books domestically, where the cost is between US$0.33 and US$0.66.46
Poor quality of products delivered to end-users: Dysfunctional health product procurement and supply chain systems are associated with an increased risk of substandard quality or counterfeit drugs, which can lead to poisoning, ineffective treatments, and anti-microbial resistance.48 It is estimated that 1 in 10 medical products in low- and middle-income countries is substandard or falsified.45 In education, some national regulatory bodies lack a reliable process to evaluate the quality of textbooks, resulting in the use of substandard materials and production and errors in the content.49 The provision of quality textbooks in the correct language should be prioritized in early grades as this is when they have the largest impact on learning. However, in Chad, a 2010 survey found that only 20% of students had a textbook in the correct language of instruction (French) in grade two, and 40% of students in grade five.46
Root Causes of These Challenges
Weaknesses in national supply chain and procurement systems in health and education have several root causes.
High production and import costs: The reasons for variations in the cost of textbooks across country and region include “fluctuating prices for raw materials, manufacturing, procurement, publishing overheads, distribution and storage, importation, and shipping.”46 In the health systems of many countries, depending on the size of the market and regulatory environment, importers and wholesalers of health products are numerous and fragmented, which significantly drives up prices. For example, there are 292 licensed medicine importers in Nigeria and 166 national wholesalers in Ghana.44
Inability to correctly predict needs: The capacity to effectively forecast procurement or requisition materials is often deficient, particularly at decentralized levels. Accurate data estimating needs and consumption rates are fundamental to the effective management of procurement and distribution processes, and yet they are often unavailable or unreliable, resulting in stock-outs or waste.44,46 In most national health systems in LMICs “there are no processes by which information about consumption is systematically captured” – with many systems relying instead on “ad hoc surveys.”44
Poor storage conditions and theft: Inappropriate distribution, storage, and usage conditions have been found in some cases to lead to an annual loss rate of 50% for textbooks. Moreover, poor security during transport and storage allows school supplies, particularly books, to be stolen and resold in the black market. A 2010 survey in Ghana found that 29% of English textbooks went missing during this process.46 Similarly, product diversion is a major driver of drug stock-outs in LMICs. The complexity of drug distribution systems can create many opportunities for diversion; in Kenya, for example, “medicines can change hands ‘five to seven times’ before reaching local clinics.”45
Inefficient transportation: The lack of a well-functioning and managed government transportation fleet is a major barrier to effective supply chains in health. Vehicles for medication distribution are often unavailable due to lack of appropriate planning, poor maintenance, and inappropriate use.44
Underlying weakness of the accountability structure: These weaknesses may be a result of fragmented responsibility and governance at different levels. Furthermore, the enforcement of supply chain and distribution regulations may be hampered by underfunding and limited human resource and organizational capacity, as well as inadequate supervision and corruption.44
Unpredictable financing: The predictability of financing for the procurement of textbooks is very important because their development, production, procurement, and distribution is a long process. However, this is the case in only a few LMICs.46 In health systems, delays in the disbursement of funds from national finance bodies or international donor agencies often result in disruptions that ripple down the supply chain.44
Policy Options for Improved Supply Chain and Procurement
There is no ‘one-size-fits-all’ approach to improving the performance of procurement and supply chain systems. There are only a few well-designed randomized or quasi-randomized studies that demonstrate effective reforms to improve health system supply chain performance. The external validity of what evidence exists is reduced by the context-specific and complex features of national supply chain systems across countries.50 Nevertheless, some promising policy avenues exist and are described below.
Option 1. Procurement from Different Actors
Working with different actors for the procurement of key inputs in health and education systems may provide opportunities to improve the performance of procurement and supply chain systems. In health systems, however, the flexibility to work across different producers may be more limited.
Regional or national production: Depending on the context and the product being procured, these may provide cost savings compared to international producers in relation to competition, taxes, import duties, and transportation. In Viet Nam, for example, the unit price for books is much lower than in many sub-Saharan African countries because it prints books domestically and fosters competition among publishers to drive down prices.46
Procurement from the private sector: Turning to the private sector for textbook procurement is something some countries have done to try to drive down costs. For example, in 2002 Uganda began working with a private publisher through a competitive process and “saw the cost of textbooks fall by two-thirds and their quality increase.”46 However, other studies in Ghana, Tanzania, and Kenya suggest that there is little effect on the inefficiency, corruption, and lack of transparency from changing from state-controlled to private sector textbook provision.51
Pooled funding mechanisms for improved predictability: These kinds of systems could provide more and predictable funding for textbooks; however, the current pooled funding mechanism for education, the Global Partnership for Education (GPE), has not had the same success as pooled funds in other sectors, such as GAVI health, in attracting more and predictable funding.46
Option 2. Re-Design the Procurement and Supply Systems
There are several potential ways to restructure these processes to make the best possible use of limited resources.
Centralized procurement and tendering processes: This can help to create economies of scale and improved purchasing power. Such reforms were found to produce cost savings in a number of case studies from different regions, including the Middle East, Brazil, Mexico, and several countries in Asia and Africa.50
Streamlined tiers of the supply chain system: Some countries have sought to decentralize procurement and supply processes to lower levels of the system, to provide additional flexibility, autonomy, and speed for purchasing at local facilities. However, in some cases, this has led to worse outcomes.44 In contrast, a quasi-randomized study in Zambia resulted in large improvements in medical product availability by cutting out the regional distribution step. Multiple modeling studies have also confirmed the benefits of reducing tiers in the supply chains for vaccines and immunization supplies.52 The decentralization of the supply of textbooks has also had mixed success with some countries, like Uganda, preferring instead to centralize procurement to combat corruption and mismanagement at the school and district levels.30
Reduced number of wholesalers or middle-men: A smaller number of wholesalers is generally preferable for optimal supply chain performance, since fewer larger wholesalers gain economies of scale in their distribution efficiency and have improved access to capital for infrastructural investments. The creation and enforcement of regulations around quality standards and distribution practices can lead to the consolidation of smaller players, although the resistance from smaller actors who stand to lose from this type of reform may be prohibitive.44 The cost of distributing textbooks can contribute to high variations in price, as seen when comparing Kenya and Rwanda. Although both countries use a commercial distribution system to deliver books, the unit textbook cost in Kenya is nearly double that of Rwanda, partly because Kenya delivers books through a bookseller middleman rather than having publishers deliver directly to schools.46
Public-private partnerships: Several effective partnerships have been established, particularly those which involve the contracting of private operators for the last-mile delivery of products. Large multinational companies partnering to improve the effectiveness and efficiency of supply chains in LMICs include Coca-Cola and the UPS Foundation.49,53
Option 3. Improved Distribution Processes
At different points in the supply chain process, improvements can be made to improve forecasting capacity, replenishment systems, as well as product transportation and traceability.
Improved stock-management and procurement request practices: Simple technology and software can be used to track consumption and demand—to know when stocks are running short and to update them faster. If such systems are not able to be put in place, particularly in areas with poor technology infrastructure or IT connectivity to carry out stock requisitioning, it is possible to combine information collection with product distribution. Such systems were found to be effective in Zimbabwe and Mozambique.44
Reduced lead-times from suppliers and increased frequency of replenishment: Increasing replenishment frequency “increases the speed and velocity of the supply chain and decreases the reliance on long-term forecasts,” approaching actual levels of demand. However, this can lead to higher transport costs, and therefore statistical modeling should be used to determine the best balance between transport costs and benefits from forecast improvement.44
Digital technologies that help “track and trace” the movement of products: In addition to improved security throughout the storage and transportation process, unique serial numbers at the package level can be a good defense against theft during the distribution chain.48 “Track and trace initiatives allow actors on a supply chain to determine where a product is at any given time (tracking) and where it came from (tracing). The approach starts with the process of serialization, in which a manufacturer assigns a unique identifier to each product that it ships using a two-dimensional (2-D) barcode that other supply chain actors can scan to obtain information about the product and record when it changes hands.” This creates a digital trail of information linking each package along its path through the supply chain for increased accountability.45
New or outsourced delivery methods: “Depending on the geography, overall economic situation, maturity of the transport market and structuring of the price and service level contracts, a third-party logistics provider can offer better service at rates comparable to the fully loaded cost of owning and operating a government fleet.” In the case of Kenya, this approach helped to address problems with transport planning, vehicle maintenance, and inappropriate use.44 Leapfrogging using novel delivery technology is also possible, such as using drone delivery for emergency supplies or deliveries in hard-to-reach areas in Rwanda.54
Option 4. Invest in Human Resources and Management Tools
Recruiting talented supply chain experts into the public sector is important for high levels of financial and operational performance. Management and leadership roles in this sector should not only be restricted to civil servants but also include individuals with strong commercial sector experience.
Professional development for procurement and supply chain professionals: Several countries have successfully implemented comprehensive short-term training programs aimed at procurement practitioners, members of tender committees, tender review boards, and oversight institutions. As procurement and supply chain processes become increasingly technology-driven, it is equally important for practitioners to also expand their expertise in business engineering and design and information technology.55 Other effective quality improvement interventions focused on improving teamwork and the human elements of supply chain management.50
Benchmarking tools to improve performance: These tools can also help to standardize supply chain performance metrics such as Data Envelopment Analysis (DEA).
Data for Decision Making Overview
Data is a fundamental part of strategic, goal-oriented, and effective systems. “Data-informed decision making” is a process that is proactive and interactive, and that “consider[s] data during program monitoring, review, planning, and improvement; advocacy; and policy development and review.”56
For data to be used for decision making, it should be accurate, timely, disaggregated, and widely available, as well as made actionable through analysis.57 Given the ambitious vision of the SDGs—with 17 goals, 169 targets, and 232 indicators to be achieved by 2030—there is a great need for quality data for monitoring and measuring progress.58
Challenges with Using Data for Decision Making
There have been gains in the frequency and quality of censuses and household surveys, however, many of the “building blocks” of national statistical systems remain weak. Importantly, this gap includes data that is central to estimating “almost any major economic or social welfare indicator—[such as] data on births and deaths; growth and poverty; taxes and trade; sickness, schooling, and safety; and land and the environment.”57 The inadequacy and unreliability of official statistics in many Sub-Saharan African countries have led to the U.N. High-Level Panel on post-2015 development goals calling for a “data revolution” to improve tracking of economic and social indicators across the developing world.59
Data in Education
Behind the learning crisis in much of the developing world is a huge data gap. Only a few middle-income developing countries have the political incentives and technical capacity to develop and sustain national data systems for education. Countries in the developing world rarely have the infrastructure of data collection in place, nor the capacity to analyze and feed information back to educators, parents, and communities. International assessments and regional initiatives cover relatively few developing countries; the majority of school children in the developing world are not tested at all. Moreover, while there is a range of data sources on education systems, services, and outcomes, these are not always translated into user-friendly formats for decision making.60
School-level enrollment statistics are necessary to make efficient staffing decisions, however, in some countries, like Kenya, this information is only available from the country’s Education Management Information System (EMIS) three times a year.59
Data in Health
Quality and timely data from health information systems are the foundation of the health system and inform decision making in each of the other five building blocks of the health system. Recent years have witnessed significant commitments to and investments in the strengthening of information systems.56 However, data quality and the availability and demand for timely analysis for decision making remain problematic.
Poor quality data: Many LMICs continue to face challenges related to the poor quality of routinely collected data. Comparing administrative and survey data of primary school enrollment in 46 surveys across 21 African countries found a bias toward over-reporting enrollment growth in administrative data—with an average change in enrollment nearly one-third higher in administrative data. “Many countries’ health management information systems (HMIS) databases rely on self-reported information from clinic and hospital staff, which aggregated up by district and regional health officers, each with potentially perverse incentives.”59
Under-resourced and under-staffed national statistical agencies: The high turnover of qualified EMIS staff, particularly in Ministries of Health, is a recurring challenge in LMICs, largely due to the low and relatively unattractive salaries.58 These agencies have also failed to improve significantly over time due to a lack of functional independence, as well as being reliant on volatile donor funding.59
Fragmented and inadequate information systems: Electronic Medical Information Systems (EMIS) in many sub-Saharan African countries are “chronically weak,” with problematic or at times absent key functions such as data entry control, import-export, data consolidation, consistency checks, and data extraction, estimation and imputations, projections, or archiving facilities.58
Limited capacity for analysis and use of data at local levels: All too often, data remains unutilized, sitting in reports, on shelves, or in databases and not being used in program development, quality improvement, policymaking, or strategic planning.56 In a survey of several tiers of Ethiopian government officials, only about 12% of officials stated that they used national information management systems as their primary source of information, preferring instead “formal field visits” (63%) or informal informational interactions such as discussions with frontline colleagues (51%) or colleagues in their organization (45%). Reliance on these more informal information sources was found to lead to only a minority of officials being able to make “relatively accurate claims about their constituents.”61
Root Causes of These Challenges
Challenges related to data for decision making are not merely technical but rather the result of implicit and explicit incentives and systemic challenges, including a lack of stable funding for national statistical systems and minimal checks and balances to ensure that the data are accurate and timely.57
Dominance of donor data priorities over national priorities: “The different needs of donors and government present trade-offs between the comparability, size, scope, and frequency of data collection. Given that donors finance a large share of spending on statistics, these differing needs can imply that national statistical systems aren’t built to produce accurate data disaggregated for use by domestic policymakers and citizens.” An example of this is the DHS in Tanzania, which reported results for seven aggregate zones that did not correspond to any practical local unit of measure or political accountability.59
Weak demand for data from users: Data are not consistently utilized by senior officials and policymakers within ministries of health and education for a number of reasons. This can be due to a lack of capacity to make data available or “because senior ministerial staff choose not to use data that contradict official views or out of fear it will damage their credibility or subject them to heavy pressure from the executive branch of government.”58
Policy Options for Data-Driven Decision Making
Option 1. Improve the Quality of Data
This can be achieved a number of ways, including through stronger systems, better monitoring, and by reducing the incentives to misrepresent data.
Better funding national data collection systems: Improving the funding levels and structure of national statistical systems and organizations could help to improve their performance. Also consider increasing domestic funding allocation for National Statistical Offices, mobilizing more donor funding through government–donor compacts, and experimenting with pay-for-performance agreements.57
Improved data collection and reporting accuracy through enhanced data audits: Facility-level technology can be used to support more frequent quality audits of routinely collected data. Regular data audits by an independent third-party verifier are a central part of PBF systems to attempt to overcome asymmetric information between the providers and payers, create accountability, and minimize gaming. Effectively targeting these verification activities can help to balance the costs and benefits of having a large enough sample to carry out effective verification activities.23
Integrating different data streams: Redesigning data systems for improved accountability could also be achieved by getting administrative and survey data to “speak to each other,” whereby household surveys can be used to provide regular checks on administrative data at different levels.59
Option 2. Strategically Selecting Data to Collect
The effort to generate data for international goals should not displace the focus from building the capacity of national statistical agencies.
Diversifying and prioritizing indicators: Health and education systems should identify and prioritize key indicators for tracking progress toward SDG targets as well as answering questions of national relevance.62,63 For measurement to promote accountability and quality improvement, it must capture the processes and outcomes that are most important to people. In many cases, data systems produce metrics that yield inadequate insight at a substantial cost both in terms of finances and front-line workers’ time. For example, a frequently used indicator is the proportion of births with skilled attendants, however, this does not adequately reflect the quality of care during childbirth and therefore may deceptively represent progress in maternal and newborn health.1
Introduce internationally recognized standard measures: Currently, few countries in the sub-Saharan African region perform international learning assessments of their students,1 and most collect learning data in a “fairly haphazard fashion.”14,60 Most school children should be able to take a test that can be compared year over year or globally benchmarked. Policymakers and citizens need a basis to assess the quality of schooling.
Option 3. Improve Demand for Data from Decision Makers
To improve the use of data at all levels, data systems and tools can be put into place.
Develop decision-maker facing data dashboards: To complement smaller initiatives to present data to decision makers, other larger dashboards or toolkits have been introduced, including the World Bank’s multidimensional Global Education Policy Dashboard and the “Data4SDGs Toolbox,” which seeks to help countries “create and implement their own holistic data roadmaps for sustainable development.”64
Data briefs or review meetings: For data to be understood and digestible by potential users, they must be synthesized and disseminated in formats that are specific and adapted to users. Different targeted information products, focusing on “need to know” information, could include standardized reports and presentation templates for regular dissemination and feedback to decision makers.56 “External briefings” were found to significantly reduce errors made by officials, particularly in contexts where organizational incentives for data use were in place.61
Targeted capacity building for data utilization: These efforts can include ministries, national institutes, academia, and other stakeholders. Better linking the data producers with data users, who may otherwise be working at different levels of the health system and have an incomplete understanding of each other’s needs and roles. By addressing barriers to data use together, producers and users of data can also identify programmatic priorities and make data available to work on them.56,59
1 International assessments and regional initiatives such as LLECE in Latin America (Latin American Laboratory for Assessment of the Quality of Education) or PASEC (Program for the Analysis of CONFEMEN Education Systems) and SACMEQ (Southern and Eastern Africa Consortium for Monitoring Educational Quality) in Africa, cover relatively few developing countries (Source: Birdsall, 2016).
Annexes
Annex 1: Summary Table of Challenges and Policy Options
Strategic Area
Major Challenges
Root Causes of the Problems
Policy Options
Human Resource Motivation and Performance
Absenteeism
Professional attrition and “brain drain”
Low technical competences in teaching and care
• Inadequate initial professional training;
• Difficult working conditions, including insufficient physical and supportive infrastructure;
• Lack of work materials and essential supplies;
• Increasing workloads;
• Low and unreliable remuneration;
• Lack of constructive supervision, professional recognition or professional development opportunities.
Option 1: Changes to payment and reward systems
• Health worker performance-based financing (PBF or P4P) schemes;
• Teacher performance pay schemes.
Option 2: Changes to recruitment and deployment:
• Higher standards for recruitment;
• Measures to attract and retain professionals in understaffed rural areas;
• Diversification of the health and education workforce.
Option 3: Enhanced professional development programs
• In-service or facility-based skills-development programs;
• Training and skills-building programs specific to management professionals;
• Technology-enabled training and support.
Option 4: Integration of technology into the classroom or the clinic
• “Blended-learning classrooms”;
• Technology for improved attendance monitoring.
Procurement, Supply Delivery and Management
Lack of availability of working materials and supplies
Inflated prices
Poor quality of products delivered to end-users
• High production and import costs;
• Inability to correctly predict needs;
• Poor storage conditions and theft;
• Inefficient transportation;
• Underlying weakness of the accountability structure;
• Unpredictable financing.
Option 1: Procurement from different actors
• Regional or national production;
• Procurement from the private sector;
• Pooled funding mechanisms for improved predictability.
Option 2: Re-design the procurement and supply systems
• Centralized procurement and tendering processes;
• Streamlined tiers of the supply chain system;
• Reduced number of wholesalers or middle-men;
• Public-private partnerships.
Option 3: Improved distribution processes
• Improved stock-management and procurement request practices;
• Reduced lead-times from suppliers and increased the frequency of replenishment;
• Digital technologies that help “track and trace” the movement of products;
• New or outsourced delivery methods.
Option 4: Invest in Human Resources and Management Tools
• Professional development for procurement and supply chain professionals;
• Benchmarking tools to improve performance.
Data for Decision Making
Poor quality data
Under-resourced and under-staffed national statistical agencies
Fragmented and inadequate information systems
Limited capacity for analysis and use of data at local levels
• Dominance of donor data priorities over national priorities;
• Weak demand for data from users.
Option 1: Improve the quality of data
• Better funding national data collection systems;
• Improved data collection and reporting accuracy through enhanced data audits;
• Integrating different data streams.
Option 2: Strategically select data to collect
• Diversifying and prioritizing indicators;
• Introduce internationally recognized standard measures.
Option 3: Improve demand for data from decision makers
• Develop decision-maker facing data dashboards;
• Data briefs or review meetings;
• Targeted capacity building for data utilization.
Annex 2: Framework for Analysis of Motivation
Source: Adapted from “Improving health worker performance: in search of promising practices” by Marjolein Dieleman and Jan Willem Harnmeijer (WHO, 2006)5
References
Kruk ME, Gage AD, Arsenault C, et al. High-quality health systems in the Sustainable Development Goals era: time for a revolution. The Lancet Global Health. 2018;6(11):e1196-e1252.
UNESCO. Education for all: the quality imperative; EFA global monitoring report 2005; summary. France: UNESCO; 2004.
Dieleman M, Harnmeijer JW. Improving health worker performance: in search of promising practices. Geneva: WHO; 2006.
Franco LM, Bennett S, Kanfer R. Health-sector reform and public-sector health worker motivation: a conceptual framework. Social Science and Medicine. 2002;54:1255–1266.
Herzberg F. One More Time: How Do You Motivate Employees? Harvard Business Review. 2003(January):10.
Chaudhury N, Hammer J, Kremer M, Muralidharan K, Rogers FH. Missing in Action: Teacher and Health Worker Absence in Developing Countries. Journal of Economic Perspectives. 2006;20(Winter):91–116.
Muralidharan K. A New Approach to Public Sector Hiring in India for Improved Service Delivery: a Working Paper. 2016.
ICFGEO. The Learning Generation – Investing in education of a changing world. International Commission on Financing Global Education Opportunity; 2016.
Cometto G, Tulenko K, Muula AS, Krech R. Health workforce brain drain: from denouncing the challenge to solving the problem. PLoS Med. 2013;10(9):e1001514.
Fritsche G, Peabody J. Methods to improve quality performance at scale in lower- and middle-income countries. J Glob Health. 2018;8(2):021002.
WHO. Global strategy on human resources for health: Workforce 2030. Geneva: WHO; 2016.
Mullan F, Frehywot S, Omaswa F, et al. Medical schools in sub-Saharan Africa. The Lancet. 2011;377(9771):1113-1121.
Evans DK, Yuan F. The Working Conditions of Teachers in Low- and Middle-Income Countries. World Bank; 2018.
WHO. The world health report 2006: working together for health. World Health Organization; 2006.
Bennell P, Akyeampong K. Teacher Motivation in Sub-Saharan Africa and South Asia. Department for International Development: Educational Papers. 2007.
Dolea C, Stormont L, Braichet JM. Evaluated strategies to increase attraction and retention of health workers in remote and rural areas. Bull World Health Organ. 2010;88(5):379-385.
Makhuzeni B, Barkhuizen EN. The effect of a total rewards strategy on school teachers’ retention. SA Journal of Human Resource Management. 2015;13(1).
Witter S, Fretheim A, Kessy FL, Lindahl AK. Paying for performance to improve the delivery of health interventions in low- and middle-income countries. Cochrane Database Syst Rev. 2012(2):CD007899.
Grover D, Bauhoff S, Friedman J. Using supervised learning to select audit targets in performance-based financing in health: An example from Zambia. PLoS One. 2019;14(1):e0211262.
Abbott P, Sapsford R, Binagwaho A. Learning from Success: How Rwanda Achieved the Millennium Development Goals for Health. World Development. 2017;92:103–116.
Mbiti I, Muralidharan K, Romero M, Schipper Y, Rajani R, Manda C. Inputs, incentives, and complementarities in primary education: Experimental evidence from Tanzania. World Bank; 2016.
Gertler P, Christel V. Using Performance Incentives to Improve Health Outcomes. World Bank Policy Research Working Papers. 2012.
Muralidharan K, Sundararaman V. Teacher Performance Pay: Experimental Evidence from India. Journal of Political Economy. 2011;119(1).
Loyalka P, Sylvia S, Liu C, Chu J, Shi Y. Pay by Design: Teacher Performance Pay Design and the Distribution of Student Achievement. Journal of Labor Economics. 2018.
UNESCO. Accountability in education: meeting our commitments. UNESCO; 2018.
KuiFunza. Teacher Incentives in Public Schools: Do they improve learning in Tanzania? Tanzania: Twaweza East Africa; 2018.
Glewwe P, Ilias N, Kremer M. Teacher Incentives. American Economic Journal: Applied Economics. 2010;2.
Barlevy G, Neal D. Pay for Percentile. American Economic Review. 2012;102.
Guajardo J. Teacher Motivation: Theoretical Framework, Situation Analysis of Save the Children Country Offices, and Recommended Strategies. Save the Children; 2011.
Ganimian AJ, Murnane RJ. Improving education in developing countries: Lessons from rigorous impact evaluations. Review of Educational Research. 2016;86(3).
Wolf S, Aber L, Behrman JR, Tsinigo E. Experimental Impacts of the “Quality Preschool for Ghana” Interventions on Teacher Professional Well-being, Classroom Quality, and Children’s School Readiness. Journal of Research on Educational Effectiveness. 2019;12(1).
Moon B. School-based teacher development in sub-Saharan Africa: Building a new research agenda. Curriculum Journal. 2007;18:355–371.
Dunsch F, Evans DK, Eze-Ajoku E, Macis M. Management, supervision, and healthcare: A Field experiment. 2017. Located at: Discussion Paper.
Jukes M, Turner E, Dubeck M, et al. Improving Literacy Instruction in Kenya Through Teacher Professional Development and Text Messages Support: A Cluster Randomized Trial. Journal of Research on Educational Effectiveness. 2016.
McAleavy T, Hall-Chen A, Horrocks S, Riggall A. Technology-supported professional development for teachers: lessons from developing countries. Education Development Trust; 2018.
ADEA. Reducing Teacher Absenteeism: Solutions for Africa. Harare: Association for the Development of Education in Africa; 2015.
Yadav P. Health Product Supply Chains in Developing Countries: Diagnosis of the Root Causes of Underperformance and an Agenda for Reform. Health Systems & Reform. 2015;1(2).
Pisa M, McCurdy D. Improving Global Health Supply Chains through Traceability. Washington, DC: Center for Global Development; 2019.
GEM. Every Child Should Have a Textbook. Global Education Monitoring Report; 2016.
Cameron A, Ewen M, Ross-Degnan D, Ball D, Laing R. Medicine prices, availability, and affordability in 36 developing and middle-income countries: a secondary analysis. The Lancet. 2009;373(9659):240-249.
IOM. Countering the Problem of Falsified and Substandard Drugs. Washington, DC: The National Academies Press; 2013.
Majeed R. Promoting accountability, monitoring services: textbook procurement and delivery, Philippines, 2002-2005. Innovations for Successful Societies; 2013.
Seidman G, Atun R. Do changes to supply chains and procurement processes yield cost savings and improve availability of pharmaceuticals, vaccines or health products? A systematic review of evidence from low-income and middle-income countries. BMJ Global Health. 2017;2.
Opoku-Amankwa K, Brew-Hammond A, Kande Mahama A. Publishing for pre-tertiary education in Ghana: the 2002 textbook policy in retrospect. Educational Studies. 2015;41(4).
Vledder M, Friedman J, Sjoblom M, Brown T, Yadav P. Enhancing public supply chain management in Zambia. Washington, DC: World Bank; 2013.
The Global Financing Facility, Merck for Mothers, Bill & Melinda Gates Foundation, and The UPS Foundation Launch Public-Private Partnership to Improve Supply Chains in Low- and Middle-Income Countries [press release]. Washington DC; 2018.
Zipline. Lifesaving Deliveries by Drone. https://flyzipline.com. Published 2019. Accessed May, 2019.
Dza M, Fisher R, Gapp R. Procurement Reforms in Africa: The Strides, Challenges, and Improvement Opportunities. Public Administration Research. 2013;2(2).
Nutley T. Improving Data Use in Decision Making – An Intervention to Strengthen Health Systems. USAID; 2012.
Glassman A, Ezeh A. Delivering on the Data Revolution in Sub-Saharan Africa – Data for African Development Working Group Final Report. Center for Global Development; 2014.
Baghdady A, Zaki O. Education Governance in Sub-Saharan Africa. Mastercard Foundation; 2019.
Sandefur J, Glassman A. The Political Economy of Bad Data: Evidence from African Survey & Administrative Statistics. Center for Global Development; 2014.
Birdsall N, Bruns B, Madan J. Learning Data for Better Policy: A Global Agenda. Washington, DC: Center for Global Development; 2016.
Rogger DO, Somani R. Hierarchy and Information. Washington DC: World Bank; 2018.
Masaki T, Custer S, Eskenazi A, Stern A, Latourell R. Decoding data use: How do leaders use data and use it to accelerate development? Williamsburg, VA: College of William & Mary; 2017.
Demombynes G, Sandefur J. Costing a Data Revolution. Center for Global Development; 2014.
This case study examines the efforts led by Minister George Werner to create fiscal space in Liberia’s education sector through a teacher vetting and testing project. By February 2018, a third-party audit confirmed that Liberia’s education ministry had removed 83% of 2,046 ghost teachers; generated US$2.3 million in annual savings; and hired 1,371 new and qualified teachers. In addition to sharing the details of this implementation success story, this case study shares reflections from key actors, highlights unique political and funding relationships, and looks ahead to what remains to be done to improve education outcomes in Liberia.
Introduction
In 2013, all 25,000 high school graduates in Liberia who applied to the University of Liberia failed the entrance exam.1 This wasn’t entirely surprising given that the average high school classroom in Liberia had 158 students; the estimated qualified teacher-to-pupil ratio ranged from 33:1 to 90:1;2 and Liberia ranked 177th out of 199 countries on the UNDP education index.3 Furthermore, more than 90% of Liberian teachers did not have a university degree and 36% were untrained and unqualified.4 So when President Ellen Johnson Sirleaf appointed George K. Werner as Liberia’s Minister of Education in 2015, he knew there was work to be done.
Werner came to the Ministry of Education with experience in the education sector. He had studied education and social work, taught at the university level, and more recently served as the head of the Liberian Civil Service Agency where he worked to clean up government payroll. In his new role, Werner knew that education outcomes were poor and that Liberia was not seeing any progress despite the amount of aid that was being received. Starting his term in the shadow of the Ebola crisis, he was primarily charged with reopening schools, setting the school calendar, and making sure teachers and students were prepared to go back to school. However, from his time at the Civil Service Agency, he knew that education was the largest and most troubled government sector and that it comprised 40% to 45% of employees on government payroll in Liberia. Looking ahead, he saw the impending likelihood of donor fatigue and realized that in order to make any significant long-term progress in improving education outcomes, he would also have to address fiscal space for education domestically.
Problem: From listening to legacy
As a trained social worker, one of Werner’s first acts as minister was to conduct a listening tour around the country. In his words, “To know a problem, you first have to assess it.” Notebook and pen in hand, Werner traveled from community to community around the country, shadowed by some staff and members of the media, to meet with parents, students, teachers, school administrators, and more. In this capacity, Werner got a first hand account of the challenges in the education system in Liberia. He learned about the day-to-day problems of different stakeholders; he learned that ‘free education’ was not really free because of uniforms and learning materials; he saw the involvement of volunteer teachers who cared more for community than their salaries; he saw what schools looked like after months of abandonment during the Ebola crisis; and more. Most importantly, however, he got a sense of what children wanted for themselves.
With this knowledge in hand, Werner put together a list of 15 priorities he wanted to accomplish during his time as minister. The top five were 1) quality learning outcomes, 2) teacher training, 3) school infrastructure, 4) free early childhood education, and 5) increasing girls enrolment and completion rates. The cost of implementing his priorities was US$100 million. At the time, Liberia’s national annual budget was US$500 million, of which US$40 to $44 million was allocated to the Ministry of Education and approximately 92% of that was budgeted for payroll expenses. Werner had no funds to put behind his priorities. The education ministry applied for a US$11 million grant from the Global Partnership for Education (GPE) to support its work over four years but GPE required that the Liberia’s domestic financing for education show progress towards reaching 20% of government budget. Werner needed to show that Liberia was taking steps in that direction.
Funding: It takes money to get money
When Werner came in to office, a pilot project (funded by USAID and implemented by FHI 360) to identify “ghost workers” and unqualified teachers was already in place. Ghost workers were defined as “teachers who never showed up for their jobs but still received pay, or who were fraudulently included on the payroll.”5 Their presence in the education system used up government budget, affected education outcomes, and affected the government’s ability to implement other programs. The pilot was being conducted in three of Liberia’s 15 counties as part of the Liberia Teacher Training Program and President Sirleaf wanted Werner to complete the removal of ghost workers across the country. This was well-aligned with a 2014 government-wide pay-reform strategy that Werner had led as part of the Civil Service Agency but also an opportunity for Werner to free up domestic funds that could be leveraged to generate more external funds and used to implement his priorities.
Werner knew that the ghost worker removal strategy would eventually free up domestic funds but it would require significant initial funds to be implemented. As such, he decided to share Liberia’s story internationally and from that a series of fortunate meetings ensued. In September 2015 at the annual United Nations General Assembly in New York City, Werner shared his plan to remove ghost workers to free up personnel costs and implement his education sector priorities with Robin D’Alessandro, CEO of Vitol Foundation. A few months later in November 2015, D’Alessandro invited Werner to speak at a conference in London. Jamie Cooper, Chair & President of Big Win Philanthropy and Dr. Muhammad Pate, CEO, were at that same conference. Cooper and Pate were intrigued by Werner’s goals. After sending a delegation to visit the education ministry in January 2016 for a feasibility assessment, Big Win approved a US$1 million grant for the ghost worker removal program as well as mandatory competency testing for all teachers. This grant was made directly to the education ministry on the condition that the Liberian government committed to reinvesting any recouped funds back into the education sector. To verify Liberia’s commitment and efficient use of Big Win’s grant, President Sirleaf authored a letter to Big Win confirming reinvestment, PricewaterhouseCoopers was brought on board as a third-party auditor, and arrangements were made to release funds on a quarterly basis (based on achieving implementation targets). This grant from Big Win was critical as the ministry leveraged it to generate additional funds to support vetting and testing across the country.
Context: The challenge of finding ghosts
In Liberia, the Ministry of Education is responsible for supervising the education sector; the Civil Service Agency is the human resources arm of the government that sets policy for pay and benefits of all government employees and informs the Ministry of Finance of personnel costs; and the Ministry of Finance makes funds available for pay and benefits. The challenge of identifying and removing ghost workers was particularly challenging because of this joint governance structure and the presence of three payrolls.
Despite the fact that Liberia’s civil war had ended more than a decade prior, its effects lingered. During the war, thousands of teaching posts were abandoned as people lost their lives or fled and often community members who stayed behind filled in. To compensate these substitute and often under qualified teachers, the government instituted a “supplementary” payroll in addition to its “regular” payroll for qualified teachers and its “general” payroll for non-teaching government employees who worked at schools.
All three payrolls were managed by the Civil Service Agency and funds were disbursed by the Ministry of Finance. The Civil Service Agency crosschecked payroll numbers with the education ministry’s formal personnel listings, however the ministry’s listings were often incorrect because the ministry had neither the capacity nor resources to verify the teacher lists it received from district and county education officers.
By the time Werner came into office, the personnel listings had not been spot checked in years, the payrolls had not been integrated, and the distinctions between the different cadres of workers were not as clear. Anecdotally, it was well known that many teachers abandoned their posts or had intermittent attendance but continued to collect paychecks. It was also not uncommon for lower level decentralized staff within the ministry to add their family or friends to personnel listings. These acts of dishonesty were magnified by flawed policies. New teachers that were hired to replace old teachers automatically took their spot on whichever payroll, regardless of qualifications or experience. This replacement policy combined with the government’s inability to check qualifications meant that unqualified teachers could get hired on the higher paying regular payroll and qualified teachers could get hired on the lower paying supplementary payroll. Furthermore, the Civil Service Agency often took months to add new names to payroll so some new teachers chose to receive their salary in the name of the teacher they were replacing to avoid any lag in payment. And to top it all off, an additional cadre of unpaid volunteer teachers had emerged.
Ultimately, the three payrolls contained duplicate names and payroll numbers, incorrect names, and missing names. All of this exacerbated the ministry’s lack of control and potential for corruption. As of November 2016, the ministry of education had 13,403 teachers on the regular payroll, 6,024 teachers on the supplementary payroll, and 7,299 unpaid teachers.6
Implementation: From planning to action
With funding in hand, the teacher vetting and testing project was officially launched in July 2016. The deadline for the project was August 2017, two months ahead of the October 2017 presidential election when President Sirleaf’s term was due to expire. Political support for this project under a new administration was not guaranteed and thus time was of the essence.
To focus exclusively on this project, a project implementation unit was created within the ministry consisting of a project manager, financial manager, field operations manager, and an administrative assistant. This unit was additionally supported by staff from the education ministry’s human resources and teacher education departments.
Appendix A outlines the specific implementation steps of the teacher vetting and testing project.
Results: Changing the status quo
The teacher vetting and testing project is the most comprehensive assessment Liberia has ever done of its education workforce. It has communicated to teachers, principals, and staff that the ministry is making an effort to keep track and hold people accountable and that abandoning one’s post will result in removal.
By February 2018, a third-party audit confirmed that almost all of Liberia’s 19,500 teachers had their qualifications vetted and 73% of them wrote the competency test. Through this process, 2,046 ghost teachers were identified, 83% were removed, and US$2.3 million in annual savings were recouped. The outstanding 17% of ghost teachers were identified in the last six months of the program and will be removed shortly leading to an additional US$800 thousand of annual savings. Gbilia noted that while reaching higher levels of domestic financing can trigger other financing options, an added benefit is a changed mindset within the ministry that they can achieve things domestically over time going forward.
As a result of the fiscal space created within the ministry’s budget and the physical spots available for hire, the ministry of education was able to hire 1,371 new and qualified teachers who were recent graduates of Liberia’s teacher training institutes that provided ministry certification. Furthermore, at least 2,000 qualified teachers who were previously on the supplementary payrolls were transitioned to the higher paying regular payroll, reducing the supplementary payroll from approximately 6,000 to 3,762 teachers. Looking ahead, the data collected has allowed the ministry to estimate that it needs to hire an additional 10,782 principals and teachers to ensure that across the country every classroom has an appropriately paid and qualified teacher. However, despite these significant successes, the last field visits conducted by the ministry found that 15-20% of teachers that had been vetted were not present. It is evident that spot checks will be necessary going forward and norms need to be eroded to communicate to staff that showing up is mandatory and that monitoring is ongoing. Essentially, teacher vetting is important but it must be accompanied by a strategic plan for robust accountability and monitoring with district and county education officers going forward.
The teacher testing component of the project yielded jarring results. Only 6% of teachers passed with a combined score on the math and English papers above 70%. Forty-five percent received a conditional pass between 40% to 69% and 49% failed with less than 40%. While these results make the challenge ahead of improving education outcomes apparent, the data will be a valuable tool for the ministry to design customized training programs to better meet their needs. Werner notes that having this evidence base within the ministry means that they are owning their own data, rather than relying on donors, and that there is intrinsic pride in this. Sheeler adds that data had always been perceived as “for donors” but ministry ownership of data has changed the way the ministry views its role in collaborating with donors. In fact, the new administration now plans to use the results of the test assessment to design its first teacher training and implement it during the next school break for teachers.
As the data continues to be analyzed, it is now becoming apparent that missteps did occur with regards to data management. The project implementation unit prioritized data consolidation but in many cases inconsistencies in data collection and formatting meant that efforts are still being made to reconcile data to create the final consolidated personnel listings. This was likely magnified because of the change in management between the pilot study by USAID and FHI 360 and the remainder of the project by the education ministry.
The results above refer to public school teachers on the regular payroll but analysis to confirm the number of ghost teachers on the supplementary payroll is ongoing. The Civil Service Agency implemented a policy that ghost workers removed from the regular payroll could be replaced but that ghost workers removed from the supplementary payroll had to be deleted. The ministry still needs to analyze how many supplementary deletions occurred so that they can reallocate those funds to hire new teachers to the regular payroll. They estimate that for every two to four supplementary ghost workers deleted they can hire one new teacher on the regular payroll, and ultimately they aim to use the data to migrate all qualified supplementary teachers to the regular payroll.
Reflections: Blinded by the urgency of the moment
Based on conversations with a number of key stakeholders with various levels of involvement in the teacher vetting and testing project, some key reflections on political risk, funding relationships, and transformational leadership emerged.
Looking back as Werner reflects on his feelings at the conclusion of his listening tour, he says, “I was blinded by the urgency of the moment. What I saw in the field pains me and blinded me to the degree that I really wanted to solve problems in the here and now.” Perhaps this naiveté was a blessing as the political risk associated with undertaking the project was much higher than the technical risk. Jamie Cooper, President and Chair of Big Win Philanthropy, comments that “George may not have appreciated the potential political risk…but the upside of that is that he was focused on changing the system and not about protecting himself.” She also notes that Werner’s relationship with President Sirleaf and his efforts to nurture it were critical to her willingness to provide political cover when needed.
The funding relationship upon which this project was built is particularly unique. Toby Eccles, Cofounder and Development Director of Social Finance, reflects that, “In a place with as few resources as Liberia, room to use imagination is extremely limited because there are only incremental changes you can make to the budget.” However, distrust of government, especially those with a history of corruption, is a common sentiment in the international philanthropic space. While the story of Liberia’s project may be appealing to other countries, a key challenge to replicating this experience within a ministry is identifying funders who are willing to give funds directly to government. One of Werner’s clear successes was his ability to attract and develop a relationship with a funder that was open to such an arrangement. While a series of fortunate events led to their meeting, Werner’s plan to campaign externally for funding; President Sirleaf’s willingness to commit in writing to reinvesting funds; and the amenability of both the Liberian government and the Big Win Philanthropy team to negotiate terms of a target-based, incremental funding deal with a third-party auditor in place are all intentional factors that contributed to this unique funding arrangement. Government efforts to recreate some of these elements may be a foundational step to generating trust and allowing such funding relationships to occur more commonly in other settings.
One critical element associated with the aforementioned funding relationship that may not be as easily replicable is the need for a transformational leader. When asked about what attracted her to Werner’s mission, Cooper immediately noted his earnest commitment. She said, “What’s more unique about George than almost any minister I’ve met is his ability to think outside the box, to try something that is really different but can have a tremendous upside.” While his leadership and public speaking skills are well admired, Werner admits that he didn’t prioritize communication domestically as much as he could have. In hindsight he would have had a better communications architecture in place and made use of ‘palava,’ traditional Liberian peace huts, to increase communication with teachers, settle disputes, and promote inclusiveness. Despite the successes, the opportunities for improvement, and the work ahead, Cooper’s final reflection on Werner is that “he resonates with integrity” – and that basic quality may be the key to why the teacher vetting and testing project worked.
Appendix A: Detailed Implementation
The following sections outlining the specific implementation steps of the teacher vetting and testing project were obtained from “Managing the Business of Education: Liberia Cleans up its Teacher Payroll, 2015-2017,” an in-depth case study by Princeton University’s Innovations for Successful Societies.7
Winning Support
The implementation team’s first challenge was to work with Gbovadeh Gbilia, Deputy Minister of Education, to secure buy-in from two crucial stakeholders: the Civil Service Agency and the National Teachers’ Association. A lack of coordination between the education ministry and Civil Service Agency was a longstanding problem, and Werner hoped his past role as head of the agency would pave the way for better collaboration.
The Civil Service Agency initially did not see the vetting project as part of its responsibility, arguing that it was up to individual ministries to ensure that personnel listings were accurate. However, because the agency had to sign off on any changes to the listing, the education ministry felt it was vital for agency officials to see the vetting process was legitimate. “In response to the initial lack of cooperation, Werner’s ministry elevated [its lobbying efforts] to another level by going directly to the finance ministry,” said David Baysah, a sociologist and education planning strategist hired to lead the vetting project’s implementation unit.
By explaining that the vetting and testing exercise could save up to US$7.5 million per year—reducing the annual amount spent by the education ministry on salaries from US$34 million to US$26.5 million—the project team secured support from the finance ministry. The team also relayed to the agency and the finance ministry that President Sirleaf had agreed up front that the funds recovered would be earmarked for reinvestment in education, and would not be put into the government’s general coffers.
Convinced by the outreach effort, officials from the Civil Service Agency agreed to have their officials accompany the vetting team as they traveled around the country. The ministry also agreed to pay additional per diems to enable staff from the Civil Service Agency who became part of the team that traveled throughout the country.
In another step to address the disjuncture between the Civil Service Agency and other government departments, the finance minister worked with the agency to introduce a policy amendment in the cabinet. Whereas the agency previously had overarching responsibility for—and substantial control over—ministry payrolls, there was now “a policy, endorsed by the cabinet, that ministries will handle their own payroll and be held accountable for it,” Baysah said. In addition to smoothing the path for the project’s implementation, the finance ministry’s creation of the draft policy promised to give greater power to individual ministries to maintain their own payrolls.
Next, the education ministry turned to the teachers’ association. In negotiations with Werner and senior officials, the association’s main concerns were that no teacher should be fired summarily based on the outcome of the competency testing, that those who failed but held at least a high school qualification should receive training, and that the government should pay adequate severance to any teachers who lost their jobs because they were determined to be “untrainable” for various reasons.
The ministry used an existing forum to open a dialogue with the teachers. Under the teacher training program that ended in 2015, the ministry had established a committee that brought together the teachers’ association, senior education officials, donor partners, and nongovernmental organizations as well as civil society groups. In response to resistance that had emerged among some teachers during the USAID pilot, the ministry framed the new project as one that would remove cheaters and improve payroll management, leading to better salaries. The team presented its plan to the committee in the hope of winning the association’s support.
Despite initial resistance, the teachers’ association’s long-serving president, Ellen Varfley, ultimately agreed to the planned vetting and testing, and the ministry agreed to provide future training opportunities to all teachers deemed trainable, and severance packages to others. In addition to being the teachers’ association president, Varfley also worked in the ministry’s teacher-training division, a position that allowed her to be involved in drafting the test.
In championing the project, Varfley said she hoped that the competency testing in particular would lead to further gains. “After doing the test, we would know if people need content or pedagogical training, which would allow us to design better training” plans, she said. “… We knew that one size does not fit all. Teachers would [ultimately] benefit by receiving better training.”
Managing Data
Before the team could begin collecting data, they needed a way to manage it. They decided to use a common software product, Microsoft Access, to create a database of information that would allow users to see the big picture as well as to focus on specific schools, districts, and counties. Data would enter the system both electronically and manually. After a teacher’s fingerprints were digitally scanned, a computer would generate a unique enrollment number. Using the same number, the team would manually upload information—including digital copies of the teacher’s qualification documents, photo, and ID materials—to the corresponding file in a database, which the team named the Payroll Data Access Tracking System.
When all the information on any particular person was in the system, “you can see the person’s face as well as all their bio data, their current status, their salary history, their health information and also all their academic credentials,” Baysah said. “It’s a one-stop shop.” The cost of setting up the system was minimal because the human resource team was able to use the ministry’s existing computer systems and worked with the ministry’s in-house IT specialist to design the platform.
Once completed, the database was a valuable management tool. In addition to forming the backbone of an integrated future payroll system, the ministry could use it for professional development and to track replacements and transfers between schools. Further, the ministry could use the database to predict how many teachers were set to retire in coming years, enabling the ministry to anticipate future costs and recruitment needs.
Gbilia’s team recognized that keeping the database up to date was crucial to its long-term effectiveness. After completion of the countrywide vetting and testing, education officers in each of the 15 counties would gain access to the database. The plan required the education officers to update the system whenever a teacher was hired, transferred, or otherwise changed status in their region. The national human resources department in Monrovia would then audit the central database every calendar quarter. The ministry’s hope was that, over time, the Access Tracking System managed by Gbilia “would not just be a data management system but also a planning system,” Baysah said.
Getting the Word Out
The team’s next task was to inform teachers about the planned project. In a nation where roads were poor and comparatively few people, particularly in isolated or densely forested rural areas, had access to television and less than half the population had cell phones,8 radio was the go-to communications medium. Aware of the need to assuage potential fears among teachers and to inform parents and the general public, the education ministry produced a series of radio spots that played on some of the more than 60 FM radio stations across the country. (Radio jingles and other productions were often used as tools to make public service announcements in Liberia). The education ministry’s radio spots aimed to head off any knee-jerk opposition among teachers by emphasizing that the vetting and testing would not lead to any arbitrary firings. At the same time, the messages reached the wider community, potentially galvanizing public support.
Prior to kicking off the vetting process in any specific county, the field team also distributed flyers at schools and engaged with community leaders and county authorities during town hall meetings. Their aim was not only to encourage public and parental support for the vetting project but to help teachers understand that they ultimately stood to benefit because the cleanup would free up more money for salaries.
“The communication was very clear that the process will lead to results and consequences: At the end of this process, teachers will have better salaries and access to training opportunities. But also, those that cannot be trained will be removed from the system,” Baysah said. “But no one will be just kicked out. … There will be severance packages.”
Public sentiment was on the side of the project team. Many parents were deeply concerned about the quality of education. Afrobarometer research network survey showed that half of all respondents felt the Liberian government handled education “very badly” or “fairly badly.”9 “When the teachers heard [the president saying that] if you want to boycott the vetting exercise or test you will be removed, protests stopped immediately,” Gbilia recalled.
The team also worked closely with local district education officers and their county-level supervisors. The local officers, who were well known in their communities, provided additional information to teachers in other areas of their counties. Before they traveled, the project unit and local education officers jointly decided on a feasible schedule and locations across a county (usually in public spaces like schools or town halls) to conduct the vetting and testing.
Vetting and Testing
Teachers from each school received assignments telling them when and where their vetting and testing would take place. While teachers were responsible for their own travel expenses, the ministry paid accommodation and food costs, as needed. The project team divided the teachers—usually about 150—into two groups. One group took the competency test in the morning, while the other group went through the vetting process. In the afternoon, the tasks were reversed. Baysah pointed out that bona fide teachers who happened to be sick on their assigned days were “provided a window for them to come to one of the other vetting venues in the county, or they would have to travel to Monrovia.”
On the assigned day, the vetting process began when school principals submitted personnel lists to the project team. The team then compared each principal’s list to lists submitted separately by district and county education officers, who monitored all schools in their areas. If principals and local officials could not explain why a name appeared on one list and not on the other, the name moved to the “ghost worker” category. This step would enable the ministry, working with the Civil Service Agency, “to get rid of some ghosts,” Baysah said. “It was the first filter.”
The competency test, designed by the education ministry’s teacher training division, contained two papers, one on mathematics and the other on English. Both tests included questions on teaching methods. The test incorporated a combination of different types of questions, including multiple choice, short one-paragraph answers, as well as one longer essay or sample lesson plan based on a prompt. Kammi Sheeler, an economist from the Overseas Development Institute (an independent London-based think tank) who worked with the education ministry on data management, noted that the ministry eventually created four different versions of the test in order to prevent cheating.
While the tests were mandatory only for salaried teachers, the ministry encouraged volunteer teachers to participate. The ministry recommended that volunteers who did well on the test but lacked formal qualifications should attend a teacher training institute and then apply for formal positions. Volunteers who scored well and held teaching qualifications would be in line to replace ghost workers on the payroll. After teachers completed the tests, the team sent the papers to Monrovia, where 25 staff members from Varfley’s teacher training division graded them. The team then uploaded the results to the digital Access Tracking System.
During the vetting part of the day, teachers formed lines behind their principals (all principals and vice principals also had their identities and qualifications reviewed as part of the project). Teachers submitted their credentials to the vetting team, including their national identity cards as well as any documents proving high school and other educational qualifications. Because some Liberians, especially in rural areas, did not have national ID documents, the vetting team also accepted voting ID cards, birth certificates, passports or driver’s licenses. “Almost everyone had at least a voting ID card, but we accepted any of these documents,” explained field supervisor Veekie Wilson.
It was particularly important to confirm dates of birth and the exact spellings of names in order to stop the practice where some teachers received salaries made out in someone else’s name. If the team identified a fake document, they seized the document, and placed the offending teacher’s name on the same list as personnel who did not show up for the vetting process. Just as was the case for teachers who missed the exercise, those who submitted fake documents were given up to two months to provide the proper documentation before their names were submitted to the Civil Service Agency for removal from the payroll.
Similarly, when the team identified a ghost worker, they submitted the name to the Civil Service Agency for removal from the payroll. The agency then sent a letter to the school where the person supposedly worked, calling on the teacher to present his or her credentials to the national education ministry. If the person in question failed to do so during a specified period, the name was removed from the payroll.
The team also regularly encountered qualified teachers who were older than the mandatory retirement age of 65. In some counties, over 10% of the teachers were eligible for pension. When a teacher was older than 65, the team issued the teacher a pensioner’s ID card from the Civil Service Agency, and the Agency official that accompanied the field team recorded that the teacher was eligible for pension. But due to a lack of funding, it often took the Civil Service Agency a long time to issue pensions and remove pensionable teachers from the payroll. In the meantime, many kept teaching to continue earning an income. (The government calculated pension benefits based on length of tenure. For example, a 65-year-old teacher with 30 years of service and a monthly salary of US$100 would get a monthly pension of about US$60).10
Project staff next made copies of all supporting documents and uploaded digital scans to the Access Tracking System. At the end of the process, teachers who submitted all of the required documents had their fingerprints scanned and were issued special biometric ID cards. (The cards were issued only to qualified teachers who also took the competency test.)
The process was not foolproof. Despite the team’s efforts to work with district and county education officers, local officials still might collude with school principals to get ghost names added to the payroll. For example, if a district and county officer, as well as a local principal, agreed to add a person’s name to their personnel listing, that person could theoretically show up and undergo vetting and testing. In an effort to curb fraud, the team carried out follow-up spot checks a few weeks after completing the vetting process, in order to identify any ghost workers who slipped through the net.
In addition, the biometric system fell short of expectations. The USAID pilot had planned to install biometric card readers at all public schools. Teachers who had been vetted could then use their biometric cards to clock in and out of work every day, reducing the opportunities available for ghosts, tracking absenteeism, and generating useful data. When the project team took over, they found that about 400 card scanners had already been purchased by the education ministry as part of the Liberia Teacher Training Program. “But we have around 3,000 public schools, so that was not enough. Many of the machines were already quite old, so we didn’t know how many still worked,” Baysah said. Another problem was that “every year you would have to pay a license fee of US$20,000 to continue using the software, but that did not include maintenance costs.”
The field team also experienced problems with the machines used to capture biometric IDs, which meant that some fingerprints were not recorded. The project team also decided not to install the 400 scanners. For those teachers who did receive IDs, the cards were still useful in proving their identities. But the money spent on the scanners was effectively wasted, and the technical problems with some data-capturing machines meant that not all teachers had their biometric information captured.
The purpose of this case study is to examine and compare evidence from five countries (Bangladesh, Chile, Ethiopia, Rwanda, Thailand) across three regions to better understand the policies and programs they have implemented towards optimizing prospects of a demographic dividend.
Bangladesh, Chile, and Thailand are already at a mature stage, while Ethiopia and Rwanda are potentially on the edge of realizing a demographic dividend in the years ahead.
Despite vast differences in geography, culture, history, industry, etc. across the five countries examined in this case study, the common denominator is their progress in reducing child mortality and fertility rates, improving female educational enrollment and attainment, as well as diversifying economic models and increased economic participation by women. Each of these factors correlates with accelerated economic development, specifically GDP per capita growth. All countries examined integrated their social sector plans into their long-term economic development plans. This suggests an underlying recognition of the importance of social sectors as drivers of economic growth.
Demographic Dividend
The demographic transition is an academic concept used to describe changing patterns of fertility, mortality, and population growth exhibited by countries around the world over the past two centuries. It is most commonly used to identify the development stage and trajectory of a country as it relates to its population structure.
In Detail: The Four Stages of Demographic Transition
Figure 1 outlines the four stages of the classical model of demographic transition.
Stage 1 (High Stationary): Characterized by a high birth rate and a high death rate. This results in slow and sometimes fluctuating population growth, which has historically been due to wars or pandemics.
Stage 2 (Early Expanding): Characterized by a high birth rate and a falling death rate, which has historically been due to increases in access to medicine, sanitation, and nutrition, and particularly driven by decreases in child mortality. This stage leads to a period of high population growth.
Stage 3 (Late Expanding): The birth rate falls towards the death rate, often due to lower child mortality from the previous stage and an increase in family planning, resulting in moderate population growth.
Stage 4 (Low Stationary): Occurs when birth rates reach the same level as death rates and population growth slows. Resources are allocated towards greater investment in fewer children, resulting in smaller, more educated families with greater workforce participation.
The demographic dividend is used to describe an opportunity for accelerated economic growth that a country can experience as it moves through Stages 2 and 3 of the demographic transition. Specifically, when birth and death rates fall in succession they give way to a bulging youth cohort in a population’s age structure. This change yields a smaller child dependency ratio, or the proportion of the population under age 15 relative to the working-age population aged 15 to 64.
During this period, assuming an appropriate policy environment, there are more people in the labor force who, because they are better off financially, generally have smaller families and more resources to invest in their children. This moment is known as the demographic dividend – a period when a country can reap rapid economic growth if it makes the right policy and investment choices. The demographic dividend tapers off when the child dependency ratio ceases to decrease and the bulging cohort ages out of the workforce.
In Detail: World Progress Through the Demographic Transition
Historically, many developed countries have experienced changes in fertility, mortality, and population growth as outlined by the demographic transition but they have varied in terms of timing and pace. Most of these countries are in Stage 4 or some may have moved into a possible fifth stage of transition where birth rates fall below death rates resulting in population shrinkage. Conversely, many developing countries are moving slowly or stalled in around Stage 3 while the least developed countries remain in Stage 2.
Figure 2: Various Stages of Demographic Transition Across the World
Within a supportive policy environment, the economic benefits of the demographic dividend are driven by three key factors: labor supply, personal savings, and human capital. Labor supply increases both due to the increase in working-age population relative to dependents and also the increase in female workforce participation that comes with decreased family size. This is magnified by the fact that workers may be more educated having been brought up in smaller families. Personal savings increase because the healthier, working-age population invests less in their children as they age, and save more to prepare for longer retirements. As the population lives longer and healthier lives, human capital becomes an asset as people deepen their investment in the health and education of their children. Also, attitudes about education, family, the role of women, and other social and political issues evolve. It is important to note that the economic benefits of the demographic dividend can only be captured if there are sufficient employment opportunities to absorb the increase in labor supply and translate it into increased economic productivity. Furthermore, the long-term implications of achieving the demographic dividend must be considered. While an increase in working-age population can drive increased incomes, it is also accompanied by an increase in public costs, as the population ages and demand for healthcare and pensions increase.
The countries examined in this case study are at different stages of demographic transition. They have achieved varying successes and encountered challenges in their pursuit of the demographic dividend (Figure 3). Rwanda and Ethiopia’s population pyramids have wide bases signaling high population growth rates and high dependency ratios. Increased access to and acceptance of family planning can narrow these bases to reduce dependency ratios and allow for a demographic dividend in the future. Bangladesh has a visible working-age population ‘bulge’ and can achieve economic benefits from it if it can further narrow the base of its pyramid with stronger family planning programs. Thailand has an older working-age ‘bulge’ that is nearing retirement fresh from completing its demographic dividend while Chile has a more streamlined pyramid that has since completed the demographic dividend, but both countries will face challenges as their ageing workforces enter retirement while experiencing longer life expectancies.
The ability of a country to achieve a demographic dividend and the extent to which it reaps economic benefits is dependent on the policy environment (Figure 4).
Figure 4: Policy Interventions Facilitating a Demographic Dividend
Source: Gribble JN, Bremner J. Achieving a Demographic Dividend. Population Research Bulleting, 2012.
Health
To facilitate the transition out of Stage 1 of the demographic transition, countries must support policies that reduce birth and death rates. Family planning is the starting point for any progress towards the demographic dividend because without it fertility cannot be effectively reduced. Men and women, especially the poor, need access to voluntary family planning information and services to avoid unintended pregnancies so they can invest more in the health and education of fewer children (Figure 5).
Ethiopia has experienced increased contraceptive use from 4.2% in 1990 to 34.2% in 2014 and reduced fertility from 5.9 children per woman in 2000 to 4.1 in 2014. A driving force behind this achievement was the implementation of the Health Extension Program (HEP) to train and deploy over 33,000 paid health extension workers to provide basic health services over 15,000 health posts in rural areas. This program has been credited with increasing contraceptive prevalence by 17% and is the foundation for Ethiopia’s Health Development Army (HDA) that promotes contraceptive use and other essential practices through social mobilization of volunteer ‘model families.’
Similarly, Bangladesh has experienced fertility declines from 6.3 births per woman in 1975 to 2.4 in 2015 which has been strongly linked to its increase in contraceptive prevalence rate (CPR) from 7.7% to 61.2% over the same time period. This progress has been largely driven by interventions such as increased contraceptive method mix, introduction of menstrual regulation, integration of maternal and child health services with family planning services at the sub-district level, increased community outreach activities to generate demand, and financial incentives to have fewer children until the mid-1990s as well as the involvement of non-state providers in the early 2000s.
Figure 5: Total Fertility (Babies per Woman) vs. GDP per Capita (US$, Inflation Adjusted), 1960 – 2015
Investments in child health are also critical because reduced child mortality motivates reduced fertility and increased desire for family planning information and services. Immunization and nutrition programs can be particularly beneficial because they address preventable illness, improve cognitive development, and prepare children to attend school more frequently, attain higher levels of education, and eventually contribute more to the workforce (Figure 6).
Rwanda has made significant progress in improving its child health, even achieving its MDG 4 goal to reduce under-five mortality by two-thirds between 1990 and 2015. One strategy it implemented to achieve this involved investing in systems-building approaches such as developing its community health workforce which now has over 45,000 community health workers (CHWs) countrywide, with one male and one female CHW providing care in each village. These CHWs are credited with implementing national prevention programs such as mosquito net provision, immunization campaigns, medical follow-ups, and family planning at the community and village levels.
While health and economic opportunity are quite interconnected, Thailand’s investment in increasing the quality of maternal and child health care along with its improving economic status in the 1980s helped significantly reduce infant and maternal mortality. The universal health insurance program that was introduced later in 2002 has been credited with increasing access to health care and reducing poverty through decreasing health spending by poorer populations and reducing families facing catastrophic illnesses.
Figure 6: Child Mortality (Under-5 Mortality Rate) vs. GDP per Capita (US$, Inflation Adjusted), 1960 – 2015
To capitalize on the changing population structure that results from reduced fertility and mortality, countries must support policies that prepare the dividend cohort to achieve maximal economic gains. Policies that increase access to education are critical for all children, particularly girls, for whom secondary school education can help delay marriage and pregnancy (Figure 7).
Rwanda has supplemented its improvements in child health by achieving near universal primary education, with net enrolment increasing by 30% to 95% between 2000 and 2015. Critical to this success is the fact that these enrollment rates are also nearly equal in terms of male and female enrolment. However, primary completion rates and enrolment in secondary and tertiary education are significantly unequal. Thailand has focused on increasing access to education in rural areas by expanding rural school coverage and rural teacher recruitment. However, Thailand continues to struggle with the quality of its education system and its graduates are generally not well equipped to compete in a knowledge-based economy.
Figure 7: Gender Parity in Education (Ratio Girls/Boys in School (%), Primary and Secondary Education) vs. GDP per Capita (US$, Inflation Adjusted), 1970 – 2014
Additionally, skills-training is essential to equip the future workforce to changing labor market needs. The type of skills-training required can change as economies grow and diversify.
Ethiopia’s Technical Vocational Education and Training (TVET) program is a good example of skills-training policy at work. TVET is a key part of the country’s capacity-building program, whose aim is to motivate entrepreneurship, create job opportunities, and train mid-level industry workers. Ethiopia aims to increase the number of trainees in its TVET program to over 600,000. Though implementation has been slow, Bangladesh also aims to support technical and vocational education but has a particular focus on increasing female enrolment and achieving gender parity in tertiary education and literacy.
Governance
As the demographic transition progresses and households become smaller and more educated, their disposable income and savings increase. Governance structures such as established legal and regulatory systems, particularly with regards to contract law and financial standards, can help attract domestic and foreign investments which can create jobs and stimulate economic growth. Conversely, systemic corruption can significantly hinder progress by diminishing trust in systems and discouraging investment. Gender equity policies, such as access to credit and property rights, can also foster the demographic transition by enabling women to achieve their desired fertility and free them up to participate in the workforce.
Bangladesh specifically aims to improve its governance through a legal aid program; enhanced integrity and corruption control regulations; improved Right to Information laws; and reforms to make the parliamentary process more effective. Ethiopia is working to improve governance by highlighting women and youth empowerment as a cross-cutting issue in its current national development plan. It aims to promote gender equity in education, employment, asset ownership, and access to capital; provide a supportive environment and financial aid for female students; increase the number of female teachers; eradicate harmful traditional practices; and improve access to capital for youth.
Chile ranks high in terms of democracy and rule-of-law which has fostered a very active private sector and supported its economic growth. It also has an independent central bank and special courts to oversee competition.
Rwanda has enshrined the importance of gender equity in its constitution and invested heavily to reach a ranking of fifth in the World Economic Forum’s 2016 Global Gender Gap Index. Nearly two-thirds of seats in Rwandan Parliament are filled by women, female labor participation is 54%, with the smallest salary gap between men and women in the world.
Economics
Effective economic policies can catalyze the demographic transition in a number of direct and indirect ways. These include labor market flexibility to respond to a diversified economy; openness to trade to bring local products to international markets and vice versa; incentives to encourage savings and investment; and physical and communications infrastructure to support domestic and international trade. Without the synergy of effective health, education, governance, and economic policies, countries cannot optimally take advantage of a demographic dividend as they move through the demographic transition.
Economic policies and programs to achieve the demographic dividend can vary based on the stage of a particular country. Rwanda and Bangladesh have implemented programs to support grassroots economic development such as Grinka (one cow per poor family) in Rwanda and “One House, One Farm” in Bangladesh which helps small hold farmers create village cooperatives to alleviate poverty and develop sustainably. Thailand’s shift from an agriculture to more industry-based economy increased economic productivity and subsequent production for export. Health insurance reduced the likelihood of workers being prevented from going to work due to illness thereby improving labor productivity. From a more outward-looking perspective, Chile has focused on reducing tariffs and signing numerous free-trade agreements to support international trade.
General Strategies
All countries examined have made an effort to integrate their social sector plans into their long-term economic development plans. Thailand included education but not health in its first two National Economic Development Plans but since the 1970s has continued to include both. This suggests an underlying recognition of the importance of social sectors as drivers of economic growth. Additionally, it suggests that they understand the intersectional nature of economic development and the role that social sectors such as health and education have to play. For example, Bangladesh explicitly states its goal of achieving the demographic dividend in its Five-Year Plan and considers its position in the demographic transition in its policy agenda.
Complementing vertical programs with horizontal, capacity-building efforts is a necessary approach. For example, Rwanda and Ethiopia have both invested heavily in human resources for health by strengthening their community health workforces. On their own investments such as these can increase the size of the health workforce, create jobs, promote health-seeking behavior, and improve health education among local populations. Arguably more important, however, is how these investments serve to support the implementation of vertical programs and magnify their potential effect. Ethiopia’s Health Development Army has even gone a step farther to actively generate demand for health care at the grassroots level. Horizontal, systems strengthening programs can be put in place at any time (even before a country is ready to capture the demographic dividend) as they can serve to support and magnify the impacts of vertical programs that are targeted to moving through the demographic transition.
Some issues that promote success do not fall into any particular sector but rather affect many sectors in different ways. These crosscutting issues need to be addressed in a targeted and collaborative way. For example, gender equity persists as an issue in primary school enrollment to secondary school attainment to age at marriage to labor force participation to access to capital and more. Tackling such an issue requires joint effort across sectors to ensure that progress made in one sector is complemented by policies in another. Gender equity is of particular importance to the demographic dividend given the potential economic benefits to increased female workforce participation, but policies to maximize this benefit must cross sectors and target females across their lifecycle. Ethiopia and Rwanda both explicitly state efforts to address gender equity in a comprehensive way while Bangladesh is more focused on tackling it within the working age population.
Subnational variation is a universal concern. High-level political commitment is necessary to drive national progress, but a top-down approach is insufficient to move the entire country forward. Inequalities between rural and urban populations as well as between the wealthy and the poor exist in every sector and can be exacerbated by policies that are not sufficiently pro-poor. Rwanda experienced this after completing implementation of its national policy in 2002 that led to reductions in infant and maternal mortality, but also increased inequality and similarly, Ethiopia’s 2010-2015 plans resulted in overall improvements, but no change in inequality.
Despite vast differences in geography, culture, history, industry, etc. across the countries examined in this case study, their progress in reducing child mortality, fertility, and improving female educational enrollment and attainment have all been correlated with economic development, specifically GDP per capita growth. Notably, all countries examined integrated their social sector plans into their long-term economic development plans. This suggests an underlying recognition of the importance of social sectors as drivers of economic growth.
The next section provides a more in-depth discussion of each country’s progress and policy efforts towards achieving the demographic dividend.
Country Cases
Bangladesh
Progress
Bangladesh is well into the demographic transition and its opportunity to take advantage of the demographic dividend is imminent. Bangladesh has already experienced decreased birth and death rates resulting in a dependency ratio of 54% and a population growth rate of 1.6% in 2014. To achieve this, Bangladesh maintained a significant drop in under-five mortality from 146 deaths per 1,000 live births in 1990 to 46 in 2015, fulfilling its MDG target.
The effect of these efforts is depicted by a bulging cohort in Bangladesh’s population pyramid that is about to enter working age. Over the next three decades, it is expected that the proportion of Bangladesh’s under-15 population will decline, the working-age population will stabilize, and the elderly population will increase as the bulging cohort moves towards old age. With declining fertility and increasing life expectancy, it is estimated that Bangladesh has a 10 to 20-year window during which to take advantage of a favorable dependency ratio.
It is estimated that by 2050 the elderly will make up almost 15% of the Bangladeshi population and old-age dependency will be greater than youth dependency.
Figure 10: Bangladesh Population Pyramids (1990, 2010, 2030)
Bangladesh has experienced declines in fertility from 6.3 births per woman in 1975 to 2.4 in 2015. In western regions (Rajshahi, Khulna), the number of births per woman has already reached replacement levels (2.1), and if current family planning methods are sustained, the national average is expected to catch up by 2025. This overall decline in fertility has been strongly linked to Bangladesh’s increase in contraceptive prevalence rate (CPR) from 7.7% to 61.2% over the same time period. However, eastern regions (Sylhet, Chittagong) experience lower levels of CPR and thus lag behind in reducing fertility.
Despite this overall progress, there have been some setbacks. Half of all teenage girls have at least one child, and early marriage remains common, with 52% of Bangladeshis married by the age of 18 – the second-highest rate of child marriage in the world. While this is a decline from 66% a few years ago, in 2017 Bangladesh relaxed the minimum marital age of 18 for women to allow for “special cases” in the “best interests” of the adolescent. There are concerns that this new legal loophole effectively reduces the legal marital age to zero.
Bangladesh has primary net enrollment above 90% and secondary enrollment close to 60%, with female primary enrollment exceeding male. On the supply side, poor quality and unskilled teachers persist as challenges. Bangladesh has a large migrant workforce that sends remittances exceeding $15 billion per year, and households receiving remittances are generally better off. However, this workforce is stunted by poor formal education, minimal English skills, and few industry-specific skills, particularly in technology, resulting in low wages and exploitative work conditions.
Policy Environment
Bangladesh has implemented Five Year Plans to drive development and growth since 1973 (except for a seven-year period from 2003 to 2010 where it switched to three-year Poverty Reduction Strategy Papers). The Sixth Five Year Plan, the first after the hiatus, spanned 2011 to 2015. It aimed to achieve 7.3% annual GDP growth but actually achieved 6.3%. By the end of this period, the poverty ratio had declined to 25%. Digital Centers for government services were established in all (approximately 4,500) Union Parishads as well as 13,000 Community Clinics to provide greater access to services for poor and rural populations.
More than 140 social safety net programs covering 25% of households have been implemented by the government and disbursed USD 1.6 billion to date. Additional programs such as “One House, One Farm,” which helps small hold farmers create village cooperatives, provides them with skill development training on management and farming, and offers grants to ultimately alleviate poverty and develop sustainably; and “Food for Work,” which since 1975 has been providing in-kind payments of wheat rather than cash to the rural poor during off-seasons for agriculture to provide them with food security and nutrition. Programs that disburse funds use e-payment systems to help recipients build credit and promote savings behavior, particularly among women.
Additional social programs that Bangladesh has implemented include “Asroyan,” which leases low-cost shelter in perpetuity to female household members; the ability to open bank accounts with only Tk 10.00 (equivalent of USD $0.125) and transfer of government assistance through those bank accounts; and the Rural Savings Bank where government contributes an equity fund equal to a household equity contribution and further matches it with a low-interest loan, thereby enlarging the trading capital of a household by three times.
The most recent plan, known as the Seventh Five Year Plan: Accelerating Growth and Empowering Citizens, covers 2016 to 2020. The key objectives of this plan are to increase annual growth in an inclusive, pro-poor, and environmentally sustainable way to 7.4% (which has since been exceeded); to reduce extreme poverty to 8.9%; and to eradicate unemployment and underemployment.
With regards to health, Bangladesh aims to reduce its under-five mortality rate from 41 to 37 by increasing immunization coverage to 100% and skilled birth attendance to 65%. It aims to reduce fertility to 2.0 by increasing the contraceptive prevalence rate to 75%. To achieve this it plans to improve service delivery and decentralization of the health system; to improve access to care for poor and marginalized populations; to improve regulations and supply to encourage public facility use (versus private); to more effectively train and deploy government-trained Community Skilled Birth Attendants; to educate the population about prevention of non-communicable diseases; to provide gender and adolescent-friendly services; and to address horizontal systemic issues such as health workforce, management and administration, finance, surveillance, drugs and equipment, and research.
For family planning specifically, key interventions include using mass communication efforts to promote delayed marriage, childbearing, and awareness of family planning methods as well as encouraging male participation in family planning decisions. (These efforts are at odds with the loophole introduced in 2017 to the Child Marriage Restraint Act that allows for younger brides and grooms in special circumstances, rather than the strict minimum marital age of 18 for women and 21 for men that was previously in place.)
With regards to education, it aims to achieve 100% net enrollment rate for primary and secondary school; to improve education quality at all levels through capacity building for teachers; to ensure 30% of primary public schools and 100% of secondary schools have a computer laboratory; and to increase grade five completion rate to 100% from 80%. The main focus to achieve the demographic dividend, however, is on secondary and tertiary education as well as vocational and technical education.
To support gender equity, it aims to achieve gender parity in tertiary education and literacy; to encourage female enrolment in technical and vocational education; and to increase female participation in government service to 25% by 2020 (though this quota has since been discontinued due to mass demonstrations but it did help female recruitment). To strengthen governance, it plans to give legal aid to at least 37,000 victims annually, enhance integrity and corruption control regulations, improve Right to Information laws, and make the parliamentary process more effective.
Bangladesh has been particularly successful at implementing policies that support sustained decrease in fertility. Between 1975 and the mid-1990s, strong political commitment supported interventions such as increased contraceptive method mix, introduction of menstrual regulation, integration of maternal and child health services with family planning services at the sub-district level, increased community outreach activities to generate demand, and financial incentives to have fewer children.
During this time period, contraceptive prevalence rate increased from 8% to 44% and total fertility rate decreased from over 6 to 3.5 children per woman. In the early 2000s, coordination between maternal and child health and family planning service providers weakened and service provision shifted from home-based delivery to clinic-based. Despite this and high contraceptive discontinuation, low use among young married women, and decreased use of long-acting and permanent contraceptive methods (LAPM), contraceptive prevalence rate increased by about 17% in four years, perhaps due to the involvement of non-state providers and the cultural legitimacy that family planning had acquired.
However, fertility decrease slowed to 3 children per woman by 2004. Similarly, since 2004 non-state providers have played a greater role than public providers and contraceptive use has exceeded 61% and fertility continues to drop. Despite its initially successful policies, Bangladesh’s current family planning program is mainly driven by short-term methods but would benefit from more LAPM and social policies to encourage delayed childbearing and wider birth spacing. Unmet family planning need remains high at 12%.
Chile
Progress
Chile has passed the period of demographic dividend and is in the mature stages of the demographic transition, facing a mostly ageing population. The combination of a declining birth rate from 23.5 per 1,000 of population in 1990 to 13.6 in 2015, and a stable mortality rate of 5.7 per 1,000 of population has resulted in a rapid shift in the population pyramid. The Economic Commission for Latin America and the Caribbean (ECLAC) estimates that Chile experienced a positive demographic bonus between 1966 and 2011. From 1990 to 2015, per capita income increased by 5.3% per year. This effect has slowed in later years with a per capita income increase between 1998 and 2008 of 0.26% per year and 0.06% in the following decade.
Figure 12: Chile Population Pyramids (1990, 2010, 2030)
From 1960 to 1990, Chile’s infant mortality rate fell 87% from 128 per 1,000 births to 16. Since then it has fallen more slowly and stagnated around 7.2 in recent years. Fertility in Chile has declined from 5.1 children per woman in 1960 to 1.8 in 2015 despite the fact that contraceptive prevalence had only reached 64% in 2006 (from 43% in 1978). Life expectancy at birth in Chile has increased by 22 years from 57 in 1960 to 79 in 2015 and the current average age of the population is 35 years. The combination of these reductions in fertility and mortality rates has led to narrowing of the base of Chile’s population pyramid, a widening upper tip, and a visible working-age ‘bulge.’
Chile has achieved near universal primary education with net enrolment at 94% in 2015, though it has decreased by 3% since 2007. Similarly, secondary net enrolment is 88% in 2015, down 4% since 2007. Gender parity in gross primary and secondary enrollment has consistently hovered around 1 since 1970.
Policy Environment
Policymaking in Chile has not been motivated by achievement of the demographic dividend, largely because the bulk of the population transition happened many years ago. However, despite working without the demographic dividend framework, Chile has implemented policies that are well-aligned with it.
With regards to health care, Chile credits its progress in maternal and child health as well as overall life expectancy to expansion of birth control access in the 1960s when the fertility rate was 4.6 children per woman; robust sanitation policies introduced in the late 1960s; and a criticized, but ultimately effective health system. Chile credits its high life expectancy to the robust sanitation policies introduced in the late 1960s and an effective, though often criticized, health system.
Chile views education as a key instrument to improving income distribution and supporting economic growth. Education quality has been an ongoing challenge for Chile in the last decade. The government has increased state spending on education through a large tax reform process. The spending has been put towards increased teacher payments, implementing teacher evaluations, providing free tertiary education, and increasing access to preschool education.
Chile has undertaken some key economic policymaking to stimulate its growth and capitalize on its demographic dividend in the last three decades. Firstly, in 1975 it implemented an outward-oriented growth strategy that involved lowering tariffs significantly and signing numerous free trade agreements. Despite the fact that this strategy was briefly interrupted between 1983 and 1985, in the last 15 years Chile has signed more free trade agreements than any other country. Secondly, Chile’s macroeconomic management has been quite successful. It has one of the lowest public debt rates among emerging markets. In the 1990s inflation was gradually reduced to approximately 3% and has remained relatively stable since then. A floating exchange rate regime has served as a buffer and strict financial regulations have maintained a healthy banking system since a large crisis in 1982. Thirdly, Chile’s financial system is more similar to a developed country’s than an emerging market with a fully funded individual account pension system that began in the early 1980s and now manages more than 90% of GDP in assets plus a banking system with assets exceeding 80% of GDP. Important institutional developments have underpinned high savings and investment. Chile has a very independent central bank that has built strong credibility and special courts carefully guard competition. Public-private partnerships have been expanded in several areas. Finally, Chile ranks high in terms of democracy and rule-of-law when compared with other countries. This has fostered a very active private sector.
Due to its economic growth, Chile was able to reduce poverty rates from 45% in 1987 to 12% in 2015. However, inequality remains an overarching theme and the Gini coefficient still stands at 47 (down from 57 since 1987). Furthermore, as the bulk of Chile’s population ages, pension is becoming an increasing concern. A quasi-universal minimum pension funded out of general taxes has helped to reduce poverty in people over 65 years of age but the middle class is facing a sudden drop in income at retirement.
Ethiopia
Progress
Ethiopia is well poised to take advantage of the demographic dividend. The narrowing base and widening stem of Ethiopia’s population pyramid reflects reductions in death and birth rates. Currently over 70% of Ethiopia’s population is under age 30 and almost 50% is under age 15. Ethiopia achieved its MDG goal by reducing under-five mortality from 203 deaths per 1,000 live births in 1990, one of the highest in the world, to 61 in 2015.
Figure 9: Ethiopia population pyramids (1990, 2010, 2030)
Fertility has declined from 5.9 children per woman in 2000 to 4.1 in 2014 and contraceptive use has increased from 4.2% in 1990 to 34.2% in 2014. Despite national progress, significant subnational variation exists. In urban areas, fertility is near replacement at 2.2 children per woman, however 81% of the population still lives in rural areas where each woman has an average of 4.5 children. Similarly, while contraceptive use has increased at the national, these changes are not uniformly reflected at the subnational level where some states (Amhara, SNNPR) experienced a six-fold increase in contraceptive use while another (Somali) experienced a decrease to only 2%. Ethiopia must find ways to replicate and sustain its progress in richer, urban areas in poorer, rural areas to maximize the demographic dividend it can achieve as a country.
Ethiopia has made significant strides in net enrolment at both the primary and secondary levels. Net primary enrolment more than quadrupled to 86% from the 1990s to 2016 while secondary enrolment has reached 31%. However, significant subnational variations persist and as well as gender disparities in enrollment and completion at the secondary and tertiary levels. This contributes to the fact that one-half of women in Ethiopia are married before the age of 18, despite it being against the law. Improving gender parity will be critical to increasing women’s workforce participation and economic productivity outside the home to ultimately maximize Ethiopia’s demographic dividend.
Policy Environment
Ethiopia launched its first ever explicit multi-dimensional population policy in 1993. The main aim of the policy was to maximize the level of welfare of the population by synchronizing the rate of population growth with that of the economy and the capacity of the country for sustained socio-economic development. As part of this effort, significant progress was made in the areas of reproductive health service delivery, population data collection and research, training, and communication. Fertility, infant mortality, under-five mortality and maternal mortality all declined. As such, the population growth rate declined and life expectancy increased. Female participation in education and access to political power and decision-making improved and a range of legal, policy, and institutional frameworks were developed and implemented on gender equity, equality and empowerment of women. Legislative measures were also taken to remove harmful traditional practices.
More recently, Ethiopia’s main development agenda is poverty eradication. To this end, it implemented A Plan for Accelerated and Sustained Development to End Poverty (PASDEP) from 2005 to 2010. The main objectives of the PASDEP were to achieve Ethiopia’s MDG targets and to ensure sustained, accelerated, economic development. Under the PASDEP, Ethiopia experienced sustained 11% annual growth in real GDP and a reduction in poverty from 39% to 30%. A key achievement was the implementation of the Health Extension Program (HEP) to train and deploy over 33,000 paid health extension workers to provide basic health services over 15,000 health posts in rural areas. This program has been credited with increasing contraceptive prevalence by 17% and reducing under-five and maternal mortality. PASDEP implementation was challenged by financial constraints resulting from inadequate official development assistance, lower than expected domestic revenues, and unpredictable rainfall.
Building on PASDEP, Ethiopia introduced the first Growth and Transformation Plan (GTPI) for 2010-2015. The guiding vision for GTPI was to eradicate poverty and become a middle-income country by 2025. To this end, its key objectives were to: (1) maintain a minimum 11% growth rate and attain relevant MDGs; (2) improve access and quality in health and education services and attain relevant MDGs; (3) achieve stability in development and democracy; and (4) achieve macroeconomic stability to ensure sustainability of growth in all other sectors. During this time period, Ethiopia achieved 10% growth and reduced poverty from 30% to 23% while maintaining similar levels of inequality (0.30 Gini Coefficient). To improve quality and access to education, programs to improve teacher development, curricula, schools, and information and communication technology were implemented while repetition and dropout rates remained a challenge. Building on the success of the HEP, Ethiopia introduced the Health Development Army (HDA), made up of volunteer families who choose to adopt the majority of the government’s 16 priority interventions (e.g. mosquito nets, immunizations, contraception use) to become certified as “model families” and act as social mobilizers to encourage similar behavior within their communities. While HEP is credited with continued increase in contraceptive prevalence, lack of research and data is a key ongoing constraint to monitoring and evaluation of Ethiopia’s family planning programs.
Ethiopia’s GTPII was developed to take forward the overarching objectives of GTPI through 2020. Key targets related to achieving the demographic dividend include halving under-five mortality rate to 30 deaths per 1,000 live births; halving maternal mortality rate to 199 deaths per 100,000 live births; increasing contraceptive prevalence rate to 55%; universal primary school net enrollment; 79% lower secondary school (9-10) gross enrollment; 45% female students in undergraduate studies; and tripling number of Technical Vocational Education and Training (TVET) trainees to over 600,000.
Key implementation strategies in education include expanding teachers from emerging regions; aligning curricula to match development goals and technological skills; increasing the number of secondary schools; and encouraging private investment to improve quality of education. Additionally, TVET is a key part of Ethiopia’s capacity-building program whose aim is to motivate entrepreneurship, create job opportunities, and train mid-level industry workers.
Key implementation strategies in health include primary care provision at all health facility levels; continued investment in HEP and HDA programs; reduction in open defecation areas and increase in households with latrines; transparent promotion ladder to reduce health worker turnover; incentives to encourage private investment in health infrastructure; and implementation of a health insurance system.
GTPII highlights women and youth empowerment as a cross-cutting issue that is required to achieve the objectives of GTPII. It aims to promote gender equity in education, employment, asset ownership, and access to capital. Additional strategies include providing a supportive environment and financial aid for female students, increasing the number of female teachers, eradicating harmful traditional practices, and expanding access to capital for youth. Women and youth development armies will be mobilized to implement cross-sectoral approaches to the challenges these populations face.
Rwanda
Progress
Rwanda has been steadily moving through the demographic transition but it is still not yet poised to capture the demographic dividend. Rwanda has made progress decreasing death rates as indicated by the wider working age cohorts on its population pyramid (compared to previous years). It surpassed its MDG target by decreasing its under-five mortality from 151 deaths per 1,000 live births in 1990 to 41 in 2015. However, the pyramid’s wide base suggests that birth rates remain too high for population growth rates to slow.
Figure 8: Rwanda population pyramids (1990, 2010, 2030)
Fertility has declined from 6.5 children per woman in 2000 to 4.2 in 2015 and contraceptive access has increased from 10% in 2005 to 48% in 2015 but still falls well short of the national target of 70%. This progress needs to be accelerated to decrease the dependency ratio and motivate increased health and education investments in children.
Rwanda has achieved near universal primary education with net enrolment at 95% in 2015, up from 73% in 2000, with near equal gender parity. Secondary net enrolment is 27% and 52% of enrollees are female. Despite traditional gender roles that women and girls continue to struggle to overcome at more local levels, Rwanda is a global leader in gender parity with 54% female workforce participation, the smallest salary gap between men and women in the world, and nearly two-thirds of Parliamentary seats filed by women. In the World Economic Forum’s 2016 Global Gender Gap Index, Rwanda was ranked fifth in gender parity.
Policy Environment
Rwanda has implemented a number of policies to achieve its rapid progress in health and education over the past two decades. In 2002, it introduced the Poverty Reduction Strategy Paper (PRSP), the national government’s first ever “systematic assessment and establishment of the actions needed to reduce poverty and generate pro-poor economic growth.” The PRSP was a four-year strategic plan focused on six priority areas: rural development and agricultural transformation, human development, economic infrastructure, private sector development, and institutional capacity building. The PRSP made good progress in social sectors such as health and education, achieving reductions in maternal and child mortality (20-30% decrease) and poverty (58.9% to 56.7%), but faced challenges in agriculture, infrastructure, and industry. Additionally, income inequality increased (0.51 to 0.52 Gini coefficient).
Building on this experience, the government introduced the Economic Development and Poverty Reduction Strategy (EDPRS 1) in 2008, a four-year strategy to target growth acceleration, job creation, and export generation through social programs such as Grinka (one cow per poor family), health insurance, and local development and rural growth programs. EDPRS 1 is credited with increasing economic growth (8.2% average), reducing poverty (56.7% to 44.9%), and reducing economic inequality (0.52 to 0.49 Gini coefficient).
As of 2013, the government is implementing EDPRS 2 with four key objectives:
Economic transformation (average GDP growth of 11.5%).
Rural development (less than 30% poverty).
Productivity and youth employment (200,000 off-farm jobs per year, increased output per worker).
Accountable governance (more than 80% service delivery, increased citizen participation).
Additionally, EDPRS 2 aims to continue to sustainably develop eight foundational elements from PRSP and EDPRS 1. Critical among these to achieving the demographic dividend are family planning (i.e. increasing access to contraceptives and reproductive health education and sensitization), education (i.e. increasing free education from nine years to twelve years and improving education quality through private sector partnership), primary health care (i.e. quality, access, and affordability of health care).
Additionally, EDPRS 2 directly addresses horizontal, systemic issues such as capacity building and gender equity that need to be addressed across all programs. For example, Rwanda has invested in developing its community health workforce and now has over 45,000 community health workers (CHWs) countrywide, with one male and one female CHW providing care in each village. These CHWs are credited with implementing national prevention programs such as mosquito net provision, immunization campaigns, medical follow-ups, and family planning at the community and village levels.
Thailand
Progress
Over the past few decades since 1970, Thailand has seen rapid demographic change. It went from a country with a high birth rate and the majority of its population below 15 years of age in the 1950s to a country that has been rapidly ageing since the late 1990s and now has a life expectancy at birth of 75 years. Thailand experienced a demographic dividend between 1975 and 2005 when the percentage of population in active labor rose from 56% in 1980 and peaked at 66% in 2005, leading to an average growth rate of approximately 0.8% per year. This bulging cohort can be seen ageing through its working years in the population pyramids below.
Figure 11: Thailand population pyramids (1990, 2010, 2030)
Thailand has seen significant progress in fertility and mortality over the last half century. Infant mortality in Thailand dropped 80% since 1960 from 102 deaths per 1,000 live births to 20 in 2000. Since then, it has continued to drop steadily and almost halved to 11 in 2016. Similarly, Thailand’s fertility rate declined from 6.2 children per woman in 1960 to below replacement level at 1.7 in 2000. The rate has continued to fall but less drastically to 1.5 by 2015 and is expected to continue to decline in the near future despite periodic policy advocates from pro-natalists.
Thailand had achieved near universal primary education with net enrolment at 96% in 2009, but enrolment dropped to 87% in 2015.
Policy Environment
While Thailand reaped a dividend from changes in its demographic structure, lack of focus on effective policy implementation (i.e. education enrollment increases vs. quality improvements) meant that the dividend was not maximized as much as it could have been.
Prior to the 1970s, health had not been an integral part of Thailand’s National Economic Development Plan (NEDP), but population reduction policies were introduced in the 3rd NEDP in 1971 as a strategy to attain sustainable economic growth. Intensive population growth-reduction policies were continuously implemented between 1977 and 1996, resulting in over 70% reduction in fertility rate to below replacement level. In addition to family planning, maternal and child health received priority focus in the overall health policy and strategies. The concomitant development of integrated health service infrastructure based on primary health care helped to improve access and health outcomes in general.
From 1975 onwards, the government began many efforts to improve equity in health starting with the indigent card policy to provide free health services to the poor. In an effort to support health systems strengthening in rural areas, village health volunteers (VHWs) were introduced in 1979 and the program has since exceeded 1 million VHWs across the country. Between 1982 and 1986, it reallocated capital investments from urban hospitals to rural areas, particularly with regards to training and employing health workers of various cadres. In 2001, it established the Health Promotion Fund using tobacco and alcohol tax to fund health promotion activities.
One of Thailand’s most significant health reforms is the establishment of the Universal Coverage Scheme (UCS) in 2002. UCS uses tax revenue to purchase health services from both public and private sectors to ensure financial risk protection for the 70% of the population uncovered by any other health insurance scheme. Since its launch, UCS has been credited with increasing access to health care for infants and women of reproductive age, especially among the poor. UCS was also found to have reduced the likelihood of workers being prevented from going to work due to illness, thereby improving labor productivity. Finally, UCS was found to reduce financial risk with an 81% reduction in catastrophic health spending between 2000 and 2009.
Thailand began systematic education investments in 1950 with the establishment of the National Education Plan. Unlike health, education investments were later integrated into the first NEDP in 1961 with a focus on increasing infrastructure to expand coverage of schools and production of teachers. Subsequent NEDPs supported education investment aimed at improving economic productivity, equity, rural expansion of schools, rural teacher recruitment, and vocational education. While rural school coverage did expand significantly, quality was not prioritized. In 1992, Thailand extended mandatory education to early secondary level (from 6 years to 9 years of school) and increased government spending in education to 20% of the annual government budget. While this increased budgetary allocation towards education has been maintained (aside from during the Asian economic crisis), quality of education continues to be a concern, particularly with regards to Thailand’s ability to compete globally in a knowledge-based economy. To this end, enrollment rates and quality in higher education and dropout rates in primary and secondary school remain an ongoing challenge.
In addition to its investments in health and education, Thailand’s economic growth has been supported by two unexpected bonuses. The first was the sharp drop in petroleum prices in 1986. The second was the reversal of the trend in exchange rates with the dollar beginning to depreciate. At this point, the government changed the basket of currencies that determined the value of the baht and increased the share of the dollar in that basket to about 90%, resulting in the baht moving down in value with the dollar. These two bonuses, along with the shift from an agriculture to a more industry-based economy, led to an unprecedented economic boom with double-digit growth rates for three consecutive years starting in 1987. During this time, concurrent booms in manufactured export goods drove industrial production, inflows of portfolio investment drove the stock market, and real estate interest drove construction and increased land prices. While the speculative bubble burst in 1991, economic growth in production continued at a rate of 7 to 8%, fueled by the industrial sector.
Sources
Admassie A, Nuru S, Megquier S. “Harnessing the Demographic Dividend in Ethiopia.” 2017. Population Reference Bureau.
Alam S. “Development Planning in Bangladesh: 7th Five Year Plan and SDG Implementation.” 2016. Government of the People’s Republic of Bangladesh.
Bloom DE, Canning D, Sevilla J. “The Demographic Dividend: A New Perspective on the Economic Consequences of Population Change.” 2003. RAND Corporation.
Bloom DE, Kuhn M, Prettner K. “Invest in Women and Prosper.” Finance & Development. 2017; 54.
“Briefing Note: The Health Extension Program” 2014. UNICEF.
Chunharas S. “Thai health system, past, present and the future.” Presentation at the MOPH executive training programme. 24 January 2018.
“Economic Development and Poverty Reduction Strategy II: 2013-2018.” 2013. Republic of Rwanda.
“Ethiopia Mini Demographic and Health Survey 2014.” 2014. Ethiopia Central Statistical Agency.
“Ethiopia’s Key: Young People and the Demographic Dividend.” 2014. Population Reference Bureau.
Graff M, Bremner J. “A Practical Guide to Population and Development.” 2014. Population Reference Bureau.
“Growth and Transformation Plan II (GTP II) (2015/16 – 2019/20).” 2016. Federal Democratic Republic of Ethiopia.
“Growth and Transformation Plan (2010/11 – 2014/15).” 2010. Federal Democratic Republic of Ethiopia.
Gruber J, Hendren N, Townsend RM. “The Great Equalizer: Health Care Access and Infant Mortality in Thailand.” American Economic Journal: Applied Economics. 2014; 6: 91-107.
“Harnessing the Demographic Dividend in Bangladesh.” 2014. World Bank Group.
Lee R, Mason A. “What is demographic dividend?” Finance and Development. 2006.
Mason A. “Overview of Demographic dividend.” Demographic Dividend Working Group. Presentation made at Barcelona, Spain. June 5-8, 2013.
Nam V, Jones F. “Inclusive Social Protection and Demographic Change: The Implications of Population Ageing for Social Expenditure in the Caribbean.” 2018. Economic Commission for Latin America and the Caribbean (ECLAC).
Pattamasiriwat D. “Labour and economic dimension.” Thailand Health Profile. Ministry of Public Health. 2012.
“Prospects for Reaping a Demographic Dividend in Rwanda.” 2014. World Economic Forum.
Roy M, Kayesh MS. “Reaping Demographic Dividend in Bangladesh: Challenges and Prospects.” Global Journal of Human-Social Science; 2016: 16.
Sagarik D. “The analysis of determinants of education expenditure in Thailand.” Dissertation in partial fulfillment of degree in Doctor of Philosophy, National Institute of Public Administration. Thailand, 2012.
“Seventh Five Year Plan FY2016 – FY2020: Accelerating Growth, Empowering Citizens.” 2015. Government of the People’s Republic of Bangladesh.
Siamwalla S. The Thai Economy: Fifty Years of Expansion. 1996.
United Nations Population Division, World Population Prospects: The 2010 Revision, low variant (New York: UNFPA, 2011).
Wagstaff A, Manachotphong W. “The Health Effects of Universal Health Care: Evidence from Thailand.” Policy Research Working Paper 6119. Washington, DC. World Bank. 2012.
Wongboonsin K. “Demographic dividend from demographic changes in Thailand.” Chulalongkorn Population Institute. 2003. (Thai language).
Dr. Karima Ladhani, Assistant Director, Program Research & Development
Dr. Michael Sinclair, Executive Director
Investments in health and health systems can create value in two distinct but related ways: by generating “value for money” and “value for many”.1 Policy makers have the opportunity to prioritize budgets in order to improve efficiency and effectiveness of health investments and expenditures thereby generating value for money, and target investments to improve equity and responsiveness to users’ needs, thereby achieving value for many.
The size of health budget and its allocation directly and indirectly impact on population health.2, 3 Low- and middle-income countries (LMICs) with similar per capita Gross Domestic Products (GDP), health expenditures as a proportion of GDP, and per person expenditure on health have different health systems outcomes in relation to population health (such as life expectancy, infant mortality, maternal mortality), financial protection (impoverishing expenditures for example) and user satisfaction.4 Beyond improvements in health system outcomes (better population health, financial protection and user satisfaction) investing in health brings distinct economic benefits for countries 5-10 and political benefits for the policymakers who choose to prioritize health to benefit citizens of a country who have electoral power.
This article draws on a framework (Figure 1) used at Harvard University’s Ministerial Leadership in Health program, to discuss questions policymakers should consider when determining how to generate greater value by prioritizing health budgets. These questions include:
What values underlie the government’s priorities for the country?
Based on these values, what goals for the healthcare system does the government hope to achieve?
Based on these goals, where should the government allocate its financial resources for health?
How should the government allocate its financial resources for health?
These questions have direct relevance for Ministers of Health, Ministers of Finance, and other ministries whose decisions impact the health systems, and can provide a shared approach when discussing and setting priorities in order to achieve government goals.
Figure 1: Framework for aligning values and outcomes when setting priorities for health
What values underlie the government’s priorities for the country?
Although a broad range of values can drive the government’s approach to resource allocation, these value sets generally fall into three broad categories: utilitarian, liberal, and communitarian, discussed below.5, 11, 12
Utilitarians
Utilitarians are consequentialists and typically focus on the value, or utility, that a decision will have. Utilitarians generally believe “the ends justify the means” (assuming “the means” involve ethical and legal decisions). Policy tools such as cost-effectiveness and cost-benefit analysis reflect the utilitarian concerns of generating the greatest outcome for the greatest number of people using the fewest possible resources – ‘greatest good for the greatest number’. Utilitarians differ in how they choose to measure total utility. Subjective utilitarians argue that value is subjective to the individual and that individuals must directly judge their own happiness for themselves. In contrast, objective utilitarians argue that individual’s choices are not always rational and that greatest impact for the available resources can be achieved by defining (and measuring) individual well-being in objective terms (for example using a universal measure or index, such as Disability-Adjusted Life Years [DALYs] and Quality-Adjusted Life Years [QALYs] to objectively measure and compare everyone’s well-being) and by agents (such as policy makers, experts) and allocating resources to maximise these measure.
Liberals
Liberals take a rights-based approach to allocation of health resources. Liberals believe that all humans have the capacity and obligation to display mutual respect to each other, and this mutual respect endows individuals with rights. Some liberals, known as libertarians, focus on negative rights, which guarantee individual freedom. For example, libertarians might focus on the rights of the individual to buy health insurance or choose their physician. In contrast, egalitarian liberals also emphasize the importance of positive rights, or a minimum level of resources and services, which can guarantee the ability for an individual to exercise his or her free choices. Accordingly, egalitarian liberals tend to favor redistribution of resources in order to ensure that the entire population has access to basic positive rights. However, with regards to prioritizing health, egalitarian liberals differ in their views on whether individuals have a right to health services (i.e. provision of and access to care) or health status (i.e. the achievement of general well-being).
Communitarians
Communitarians do not focus on the level of the individual in assessing a policy, but rather on the level of the community or society. As such, communitarians evaluate the merit of a policy based on whether it adheres to a community’s value set and whether the policy promotes a society consistent with that value set. Communitarians would typically oppose a health policy which achieved positive population health outcomes with an intervention that defied local cultural norms or values. Communitarians fall into two broad categories: those who believe in a single set of values which would promote a better society (universal communitarians), and those who argue that each society should set its own values and norms based on the context-specific factors (relativist communitarians).
These value sets are not mutually exclusive. Policymakers might include both a utilitarian and communitarian perspective in an analysis where they prioritize health interventions based on their objective utility but exclude any that overtly defy local norms. Further, governments can modify their ethical values as they learn more about a population’s needs and their ability to meet those needs. However, it is important to maintain adequate “coherence and explicitness” when articulating one’s values; doing so creates transparency for the population and gives others the opportunity to agree with the government’s choices because they can understand the rationale behind these choices.
Based on these values, what goals for the healthcare system does the government hope to achieve?
Policymakers must consider which outputs and outcomes to prioritize when allocating resources for health. In this context, the term outputs refers to how well the health system performs its delivery of personal and public health services to the population, whereas outcomes, refer to the ultimate goals the health system aims to achieve. These goals include health status, financial protection, and user satisfaction. In many cases, strong delivery of health systems outputs is necessary but not sufficient for strong performance in relation to health system outcomes.
A policymaker needs to balance four key objectives for the outputs achieved by a health system:13
Equity refers to the differences in how a policy affects people of different groups. An analysis of a policy’s “vertical equity” takes into account its differential impact across different populations (e.g. income or wealth levels, or different diseases), whereas an analysis of “horizontal equity” looks at whether the policy treats individuals at the same income level (or individuals that are similarly situated in relation to a health problem) the same.5
Efficiency has been defined many ways in the fields of policy analysis. For the purposes of health systems analysis, we draw on economic definition of technical efficiency, in which society is producing the most goods and services for the least cost.5
Effectiveness refers to whether interventions are evidence-based and safe.13 In other words, an effective intervention will achieve the desired health outcomes.
Responsiveness refers to whether the health system meets the public’s legitimate non-medical expectations. Responsiveness is a highly subjective measure and depends on the perceptions among citizens of a health system’s functioning. 14
Policymakers’ values will influence which health system outputs they prioritize. For example, pure utilitarians will likely care most about efficiency and effectiveness, to achieve ‘value for money’, and they will less likely prioritize equity. They might also disregard the importance of responsiveness as an objective, unless they believe that a health system’s responsiveness generates value for the population. Liberals, who focus on individuals’ rights, will prioritize equity and responsiveness of the system, to achieve ‘value for many’, with libertarians emphasizing the importance of responsiveness (for example choice of health service providers) and egalitarian liberals emphasizing equity in access to positive rights (e.g. basic health services and medicines). Communitarians, who emphasize society’s values, will prioritize the objectives most relevant for achieving the best possible society. Accordingly, they will likely emphasize responsiveness and equity of the system at a societal level, although the emphasis could vary depending on the specific values of the society.
In addition to setting output objectives, policymakers must also pay attention to the health systems outcomes, or the overall goals, these outputs produce for a country’s health system: 5, 13
Health status refers to the actual health of a population. Measurements of population health status include life expectancy, burden of disease, mortality rates for specific groups (e.g. infant mortality and maternal mortality), and prevalence of specific diseases.
Financial risk protection refers to helping people avoid large and unpredictable payments for health, also known as catastrophic (or impoverishing) expenditures. Mechanisms to provide financial risk protection typically involve insurance schemes with risk-pooling functions, or tax funded health systems where services are typically ‘free’ or have low levels of cost sharing at the point of care delivery.
Citizen satisfaction refers to the degree with which users of the health system rate the system as satisfactory.
As with outputs, health systems outcomes also derive directly from the values described earlier. For example, objective utilitarians might concern themselves most with the population’s average health status, whereas egalitarian liberals might focus most on the distribution or range of health statuses in the population (as a measure of equity levels). Egalitarian liberals will also emphasize the importance of financial risk protection as a means for ensuring economic opportunities for all. Subjective utilitarians might place a high value on citizen satisfaction, as would libertarians (in the sense that satisfaction relates to an individual’s level of choice.)
Based on these goals, where should the government allocate its financial resources for health?
Once the government has identified its objectives for the outputs and defined its goals for the health system, it can invest in specific programs or interventions accordingly. A health system has four main functions which a government can prioritize for investment: 13
Governance and organization encompasses the organizations and institutions involved in delivering products and services to citizens15 such as hospitals, primary care clinics, and supply chains which provide medicines to providers. A government could choose to invest in the governance and organization of the health system by improving accountability, increasing transparency of decision making, updating management policies for health facilities, changing the referral network of the system, or improving processes for decision-making at the programmatic level.
Health financing involves mobilizing, pooling and allocating financial resources. Funds can be mobilized through taxes, insurance or direct out-of-pocket payments, pooling could be achieved through pooling of contributions by the government or through insurance schemes – such as social health insurance, and community-based health insurance.3 A government could choose to invest in health financing by creating a new insurance scheme, expanding coverage of existing insurance to new patient populations, or by expanding the range of services covered under existing schemes. Finances can be allocated using budgets or other provider payment methods linked to individual patients (per capita payment), activity (fee-for-service or case mix payments), or outputs (performance related pay for achieving targets for example)
Resource management entails overseeing the inputs, such as human resources and labor, pharmaceuticals, and medical technologies, that are used to produce outputs, for example provision of personal health care or public health services,. 15 The government can invest in the management of resources by purchasing these resources (e.g. by procuring medicines or by employing or contracting doctors), or by improving systems that oversee resources (e.g. budgeting tools, and health information systems) or that deliver them (e.g. through supply chain management systems) or by investing in infrastructure and human resources to strengthen health system by developing primary health care which enhances allocative and technical efficiency, improves population health outcomes at lower cost, achieves equity and improves user satisfaction. 16
Personal healthcare and public health services refer to all of the activities actually involved in delivering care to patients. Strong health systems enable delivery of these services. Governments also invest in specific services that generate value for money and value for many – for example by investing in primary health care to deliver highly cost effective interventions that have population impact. Several investment cases have been made for “good buys” that can be delivered in an integrated manner at primary care level in an efficient and effective way, for example those identified by the Lancet Commission on Investing in Health 17; UNAIDS HIV Investment Framework 18; STOP TB Strategy 19; the Global Strategy for Women’s and Children’s Health spearheaded by the UN Secretary General 20; interventions identified in the Global Malaria Action Plan 21, and; the Package of Essential Noncommunicable Disease Interventions (also known as WHO-PEN) 22.
How should the government allocate its financial resources for health?
There is no formula for determining which health interventions or areas to prioritize, and while important limiting analyses to comparisons of cost-effectiveness is insufficient for policy making as values an priorities need to be considered carefully for each country.
Without universal consensus on the principles for prioritization, governments need to adopt an approach to make resource allocation decisions and justify their policies.23 Accordingly, ethicists at Harvard University have proposed a framework known as “accountability for reasonableness” (A4R) to guide this decision-making process. A4R which is a process grounded in democratic principles aimed at legitimizing decision-making among “‘fair-minded’ people who seek mutually justifiable terms of cooperation” has four conditions 24:
Publicity condition: Decisions that establish priorities in meeting health needs and their rationales must be publicly accessible.
Relevance condition: Policymakers should provide reasonable rationales which appeal to evidence, reasons, and principles accepted as relevant by fair-minded people when justifying their decisions. Rationale should be relevant for a broad range of stakeholders in decision-making.
Revision and appeals condition: There must be mechanisms for challenge and dispute and, more broadly, opportunities for revision and improvement of policies in light of new evidence or arguments.
Regulative condition: There must be public regulation of the process to ensure that conditions 1, 2, and 3 are met.
While A4R does not identify the priorities for government investments, it establishes a transparent deliberative process for publicly and legitimately determining these priorities in order to guide investment decisions. The principles of A4R have influenced priority setting for health in several places such as: UK, where the National Institute for Health and Clinical Excellence (NICE) takes social value judgments into account when making recommendations about coverage for new treatments 25; Mexico, where decisions about which diseases the public catastrophic insurance should cover involve working groups that evaluate the clinical, economic, ethical, and social considerations 26; and Oregon where, in 2008, a Health Fund Board made a plan to insure all legal residents of the state involving a wide group of stakeholders and extremely transparent decision-making / information-sharing 27.
The impacts of Government Health Spending
Health system outcomes
Changes in government health spending can directly impact on cause-specific mortality. For example, in low-income countries a 1% decrease in government health spending is associated with an increase of 18 deaths for every 100,000 live births in the neonatal period and 98 deaths before the age of five for every 100,000 live births, controlling for populations size, population structure, and inter-country differences in health care infrastructure. The statistical significance of this result holds even when controlling for economic conditions, infrastructure, infectious disease rates, and private health spending rates. 28
From 1999-2004, a 10% increase in per capita total health expenditure was associated with a 22% reduction in infant mortality rate and 10% increase in per capita public health expenditure was associated with a 21% infant mortality rate. 29 Globally, a 1% increase in government health spending is also associated with a significant decrease in cerebrovascular deaths.30
Increasing government health spending and improving the efficiency of spending can further overall life expectancy in a country. 9 For example, among nations below the regional average for GHS, increasing government health spending to the regional average would improve health adjusted life expectancy (HALE) by:
1.2 years in Africa
0.9 years in Asia / Pacific
4.1 years in Middle East / Central Asia
In addition, among nations below the regional average for efficiency in government health spending, increasing efficiency to the national average would result in an increase in HALE by:
1.5 years in Africa
1 year in Asia / Pacific
1.3 years in Middle East / Asia
Achieving the health systems goal of financial risk protection through universal health coverage (UHC) can also improve population health status. Cross-country analysis on the influence of insurance coverage on health outcomes suggests that financial coverage has a causal influence on health, especially for low-income individuals, who gain better access to necessary care when they receive coverage. 31
Examination of individual countries’ experiences implementing UHC supports this finding. For example, Thailand’s Universal Coverage Scheme included benefits such as inpatient and outpatient care, surgery, accident and emergency visits, dental care, diagnostics, prevention and health promotion, and medications, and universal coverage increased utilization of many health services, including inpatient and outpatient visits. 32, 33
Universal Health Coverage in Turkey rapidly expanded family medicine centered primary health care to improve ratio of nurses and physicians to patients across the country to address unequal distribution of human resources which helped to expand access to maternal and child health services, and resulted in a significant decrease in infant mortality and narrowed gaps in health outcomes between the rich and the poor. 13
Similarly, across many Latin American countries, where health has been established as a constitutional or legal right, several countries such as Brazil have expanded primary care as part of the platform universal health coverage, for improving efficiency of health budgets and to achieve equitable access to healthcare services. 34 The expansion of universal health coverage has led to significant declines in infant mortality, under-5 mortality, and maternal mortality across most Latin American countries between 1990 and 2010. 34
Economic outcomes
Evidence strongly suggests that improved population health has positive economic impacts for a country. Government health spending positively impacts on population health, and provides a sound “return on investment” in the form of stronger economic output and economic growth for the country. Evidence for the linkage between health and increased economic output exists at both the microeconomic and macroeconomic level.
Box 1. Case study of investments in antiretroviral treatment
Expenditures on antiretroviral treatment for people living with HIV/AIDS provide a useful case study of a health investment with significant health and economic returns. 39 By the end of 2011, 3.5 million patients were receiving antiretroviral treatment co-financed by the Global Fund, and 80% of those patients lived in 20 African countries. The total cost of treating these patients from 2011 to 2020 was estimated at $14.2 billion. This health investment was projected to save up to 18.5 million life-years. Further, the investment was estimated to yield up to $34 billion in economic benefits (for a net benefit of up to $19.8 billion) through three primary channels: $31.8 billion in labor productivity improvements, $0.83 billion in orphan care costs averted, and $1.4 billion from the delay of end-of-life care.39
Microeconomic Impact
At the microeconomic level, better health can improve the financial prospects for individuals and households. 6 In particular, malnutrition, frequent illness, and an unstimulating home environment can limit the physical and cognitive development of a child. Conversely, proper nutrition and health allows for the adequate physical development of children and improved performance in school. Thus, investments at an early age “help to raise the potential for long-term academic and workplace success and lifelong well-being.” 6
Interventions targeting specific diseases and conditions, such as deworming for school children, iron supplements and iodine to treat malnutrition, and malaria prevention can all lead to improved education or income outcomes for individuals. 7 Among working individuals, illness can have direct, negative consequences for their income. The mechanisms linking ill health to reduced income and wealth include impoverishing health expenditures, reduced education opportunities, decreased productivity at work, long-term separation from the work force, and disengagement from other economic activities.
Macroeconomic Impact
Macroeconomic evidence also supports the idea that investing in health generates positive economic returns.7 In particular, there are four channels through which investments in health might improve the overall economic state of a country, corroborated by the microeconomic evidence described above:
Labor Productivity: Ceteris paribus, a healthy workforce will have higher labor productivity than an unhealthy workforce due to increase energy and reduced illness-related absenteeism, whereas illness in an individual can lead to loss of income, impoverishing expenditures, reduced productivity and loss of employment.
Educational Opportunities: A healthy population has increased educational opportunities, and education levels have a direct impact on income growth for a country.
Savings and Working Years: Populations with high life expectancies will tend to save more for the future and likely will have more working years. These increased savings can lead to increased investable capital, an important driver of growth.
Demographic Dividend: Health investments that change mortality rates and total fertility can lead to a “demographic dividend,” in which the ratio of working-age to non-working-age people in the country increases and productive capacity increases on a per capita basis. Assuming that the country has or can create certain conditions to enable productivity of this working-age group (e.g. proper educational opportunities), the country will experience a “demographic dividend” that leads to its growth. This demographic dividend accounts for up to one-third of the economic boom that many East Asian countries experienced between 1965 and 1990.
Political outcomes
The process of formulating health policy and allocating resources to health depends on the political structure and climate of a country, and, as such, has implications for the country’s political outcomes. For example, the transition towards universal health coverage (UHC) has had distinct positive political benefits in many countries over the last several decades. 35 In addition, health policy in countries such as Turkey, the UK and Brazil has significantly influenced political landscape and political outcomes.
In Turkey, after a regime change in 2002, the government implemented a Health Transformation Program (HTP) with significant commitment from the political leadership of the country, and this transformation led to increased levels of public satisfaction with the government (Box 2) 13, 36 and have influenced voter intentions in favour of the government.i
After the re-democratization of the Brazilian government, the 1988 constitution formally defined health as a “citizen’s right and obligation of the state” and established the Unified Health System (SUS), which sought to unify the fragmented care delivery network into a national health system under the purview of the MoH. 37 Today, 75% of Brazil’s population, or 195 million people, receive services and coverage from SUS. 38
Box 2: Turkey’s Health Transformation Program
In the 1990s, Turkey faced three distinct but related problems related to its health system: inadequate and inequitable financing of the system, an absolute shortage and inequitable distribution of physical infrastructure and human resources, and disparities in health outcomes, especially between the east and west.13 Under-5 mortality rates in 1998 were 75.9 deaths per 1000 live births in the less-developed east and 38.3 deaths per 1000 live births in the more developed west. A major earthquake in 1999 left 17,000 dead and another 500,000 homeless, exposing major faults in the government’s ability to respond to emergencies and deliver services.
Turkey’s 2002 elections resulted in a majority for the Justice and Development Party, ending a decade of ineffective coalition governments. In 2003, as part of a broader objective to improve the economy and welfare, the Ministry of Health (MoH) introduced a Health Transformation Program (HTP) to help achieve UHC. Motivation to enact these changes, including improvements in the health system, came directly from public pressure, and a failure to achieve these goals would have resulted in public backlash. 36 Further, the public expressed high levels of dissatisfaction with the health system, with only 39.5% of people indicating they were satisfied with quality of care in 2003. Accordingly, the government displayed high levels of political commitment to this effort, with the Minister of Health visiting 81 provinces at the beginning of the HTP to meet with local government and agree to HTP implementation plans.
The HTP aimed to address several health system challenges, including organization, financing, service delivery, human resources, and pharmaceuticals. The government adopted a flexible approach when implementing HTP, combining incremental and tactical changes, with high visibility to citizens, with long-term, strategic shifts that required structural changes to the system. A transformation team continuously monitored progress of the HTP; with an emphasis on citizen satisfaction with the transition, conducting focus groups, stakeholder analyses, and annual household surveys.
The HTP led to significantly improved access to and usage of health services, resulting in improved health outcomes on a number of important measures such as infant and maternal mortality. User satisfaction with quality of care also increased to 79.5% by 2011. The successful rollout of HTP served as a blueprint for the expansion of other social services by the Turkish government, and public satisfaction with the process contributed to the government’s re-election in subsequent years.
In the UK, the National Health Service (NHS) receives broad public support, with 89% of the public agreeing with the idea of a tax-funded national health system, which is managed by the government. However, projections show that by 2030, the NHS will have a £65 billion funding gap. Therefore, UK policymakers will have to balance the competing health, financial, and social demands placed on the NHS in order to maintain its relevance going forward.
Conclusion
This article aims to introduce a framework for policymakers to consider how their values influence priority setting for health, and the potential impacts that these priorities will have on health systems, economic, and political outcomes.
By clearly articulating values and priorities, policymakers can develop a transparent and deliberative process to better discuss and engage their constituents in health systems decisions and to set priorities that create greater value for money by improving efficiency and effectiveness of budget allocation decisions and more value for many by enhancing equity and responsiveness in the health system.
References
Atun, R., The National Health Service: value for money, value for many. Lancet, 2015. 385(9972): p. 917-8.
Etienne, C., A. Asamoa-Baah, and D.B. Evans, Health systems financing: The path to universal coverage. 2010: World Health Organization.
Gottret, P.E. and G. Schieber, Health financing revisited: a practitioner’s guide. 2006: World Bank Publications.
The World Bank. Indicators. 2015 [cited 2015 March 23]; Available from: http://data.worldbank.org/indicator. http://data.worldbank.org/indicator
Roberts, M., et al., Getting health reform right: a guide to improving performance and equity. 2008: Oxford university press.
Jack, W. and M. Lewis, Health investments and economic growth: Macroeconomic evidence and microeconomic foundations. World Bank Policy Research Working Paper Series, Vol, 2009.
Bloom, D. and G. Fink, The economic case for devoting public resources to health. Manson’s Tropical Diseases, 2013: p. 23-30.
Atun, R. and S. Fitzpatrick, Advancing Economic Growth: Investing In Health. A summary, 2005.
Grigoli, F. and J. Kapsoli, Waste not, want not: the efficiency of health expenditure in emerging and developing economies. 2013.
Cutler, D.M., A.B. Rosen, and S. Vijan, The value of medical spending in the United States, 1960–2000. New England Journal of Medicine, 2006. 355(9): p. 920-927.
The World Bank. How do national health systems reflect the country’s and the community’s values? 2011 [cited 2015 December 7].
Roberts, M.J. and M.R. Reich, Ethical analysis in public health. The Lancet, 2002. 359(9311): p. 1055-1059.
Atun, R., et al., Universal health coverage in Turkey: enhancement of equity. The Lancet, 2013. 382(9886): p. 65-99.
World Health Organization, The World health report: 2000: Health systems: improving performance. 2000.
Hsiao, W.C., Abnormal economics in the health sector. Health policy, 1995. 32(1): p. 125-139.
Jamison, D.T., et al., Global health 2035: a world converging within a generation. The Lancet, 2013. 382(9908): p. 1898-1955.
Schwartländer, B., et al., Towards an improved investment approach for an effective response to HIV/AIDS. The Lancet, 2011. 377(9782): p. 2031-2041.
Raviglione, M.C. and M.W. Uplekar, WHO’s new Stop TB Strategy. The Lancet, 2006. 367(9514): p. 952-955.
Ki-Moon, B., Global strategy for women’s and children’s health. New York: United Nations, 2010.
Roll Back Malaria, The global malaria action plan. Roll Back Malaria partnership, 2008.
World Health Organization, Package of essential noncommunicable (PEN) disease interventions for primary health care in low-resource settings. 2010.
Daniels, N., Accountability for reasonableness: Establishing a fair process for priority setting is easier than agreeing on principles. BMJ: British Medical Journal, 2000. 321(7272): p. 1300.
Gruskin, S. and N. Daniels, Process is the point: justice and human rights: priority setting and fair deliberative process. American Journal of Public Health, 2008. 98(9): p. 1573.
Daniels, N. and J.E. Sabin, Accountability for reasonableness: an update. BMJ, 2008. 337.
Daniels, N., Accountability for Reasonableness in Developing Countries, in Just Health: Meeting Health Needs Fairly. 2007, Cambridge University Press: Cambridge.
Daniels, N., Decisions about access to health care and accountability for reasonableness. Journal of urban health, 1999. 76(2): p. 176-191.
Maruthappu, M., et al., Government Health Care Spending and Child Mortality. Pediatrics, 2015: p. peds. 2014-1600.
Anyanwu, J.C. and A.E. Erhijakpor, Health Expenditures and Health Outcomes in Africa*. African Development Review, 2009. 21(2): p. 400-433.
Maruthappu, M., et al., Unemployment, government healthcare spending, and cerebrovascular mortality, worldwide 1981–2009: an ecological study. International Journal of Stroke, 2015.
Moreno-Serra, R. and P.C. Smith, Does progress towards universal health coverage improve population health? The Lancet, 2012. 380(9845): p. 917-923.
Hanvoravongchai, P., Health financing reform in Thailand: toward universal coverage under fiscal constraints. 2013.
Limwattananon, S., et al., Why has the Universal Coverage Scheme in Thailand achieved a pro-poor public subsidy for health care? BMC Public Health, 2012. 12(Suppl 1): p. S6.
Atun, R., et al., Health-system reform and universal health coverage in Latin America. The Lancet, 2014.
Yates, R. and G. Humphreys, Arguing for universal health coverage.
Atun, R. and S. Sparkes, Fixing a Broken Health System: Confronting Health System Challenges in Turkey. Harvard School of Public Health: Executive and Continuing Professional Education: Boston, MA.
Couttolenc, B. and T. Dmytraczenko, Brazil’s primary care strategy. 2013.
Kepp, M., Upcoming election could rekindle health debate in Brazil. The Lancet, 2014. 384(9944): p. 651-652.
Resch, S., et al., Economic returns to investment in AIDS treatment in low and middle income countries. PloS one, 2011. 6(10): p. e25310.
Dr. Rifat Atun, Professor of Global health Systems, Director of Global Health Systems Cluster, Harvard T. H.
Chan School of Public Health, Harvard University
Gabriel Seidman, Doctor of Public Health candidate and Centennial Fellow, Harvard T. H. Chan School of
Public Health, Harvard University
Efficient and effective health systems are critical for managing healthcare costs. In low and middle income countries (LMICs) of Africa, Asia, and the Middle East, increasing the efficiency of health spending could increase health-adjusted life expectancy by 1-2 years.1 Effective management of human resources and competent procurement and supply chain management of medicines, which together account for the largest costs in any health system, are critical for improving health systems efficiency.
Task shifting enables more efficient use of the human resources2 and can produce equivalent or superior outcomes for many diseases and health interventions including non-communicable diseases,3 HIV/AIDS,4,5 contraceptive distribution,6 and others.7 Community health workers can accelerate task shifting and to close the gap in healthcare access in LMICs.8 Improved procurement and supply chain management can reduce costs and diminish drug shortages,9 which adversely affect health outcomes especially in LMICs with weak procurement and supply chain management systems.10
Task shifting
Evidence strongly points to benefits of task shifting, which can reduce health costs to the health system or the patient with 6.9% to 98% reduction in costs per patient treated or overall programmatic costs. The benefits of task shifting to CHWs are demonstrated when managing general health system activities11 or specific conditions. Management of tuberculosis, which leads to 1.5 million new cases worldwide each year12 and requires medication under supportive observation for many months,13 has been shifted to health workers in the community with 57–74% reduction in the cost per patient treated in Ethiopia, South Africa and Uganda, and by 32–44% in Bangladesh and Pakistan.14–19 In Brazil supervision of medication has been shifted to close relatives with reduced program costs,20 or in Bangladesh entrusted to patients.21
For HIV/AIDS where around 15 million people receive life-long antiretroviral treatment (ART) and require regular follow up to monitor response,22 task shifting has produced cost savings without adverse effect on care. In China, community based detection of HIV in high-risk groups led to a 97% reduction in cost per case detected.23 In Ethiopia treatment initiation and monitoring of ART was shifted from physicians to nurses with cost savings.24 In Nigeria shifting ART care to less expensive cadres of health workers lowered costs,25 and in South Africa and Uganda moving dispensing of ART from pharmacists to pharmacy assistants reduced human resource costs.26–28
Task shifting has also produced cost savings while maintaining service quality for surveillance and treatment of malaria,29,30 controlling blood pressure,31 management of acute malnutrition,32 detection of sleeping sickness,33 treatment of mental illness,34 management of major obstetric procedures,35 treatment of severe pneumonia in Pakistan with 81% reduction in costs,36 surveillance to reduce transmission of Chagas disease,37 and diagnosis and treatment of schistosomiasis.38
Supply chain management and procurement
Improved procurement and supply chain management has enabled different countries to reduce drug prices by 7.7% – 79.4%, increase drug availability and to reduce drug stock outs. Brazil has introduced national policies to promote multiple sources for procured drugs, develop national pharmaceutical industry, and improve procurement. Between 1997 and 2003 Brazil achieved an 80% reduction in the annual cost of antiretroviral drugs.39 In India, development of an essential drugs list, centralized procurement, and promotion of rational drug use among physicians resulted in around 30% cost savings and increased drug availability.40 The National Essential Medicines Scheme in China created an essential medicines list, improved public procurement of drugs, and achieved cost savings of up to 40% for patients in rural districts.41
Centralized or pooled procurement of drugs has produced significant cost savings, as shown by group purchasing by neighboring countries in the Middle East,42 by different government agencies in Jordan,43 by different municipalities in Brazil,44 or by hospital networks in Serbia and Brazil.45,46 Centralized procurement by Mexican government has lowered drug prices for ART by 38%, but not as much as benchmark prices obtained by other upper middle-income countries.47,48 Centralised procurement can have unintended consequences. In Kenya, centralised procurement for anti-malarial medicines resulted in increased stock outs, as the sole supplier selected could not meet demand.49 Procurement of locally procured drugs can also lower costs, but not always as monopolies emerge.50
In LMIC, better supply chain management improves drug availability and reduces stock outs, including in disaster settings,51 for primary care drugs,52–54 for contraceptives,55 for drugs related to HIV care other than antiretroviral medicines,56 and reduces energy costs associated with the supply,57 though minor increase in procurement costs could occur.58
Revolving drug funds, where users make an initial financial contribution for procuring drugs and regular re-stocking of supplies, which users then pay to purchase,59 can produce cost savings when introduced with enhanced procurement or supply chain management, as shown in Sudan,60 or improve drug availability, as shown in Guinea61 and Nigeria.62
Innovations in financing and supply chain management, such as the Affordable Medicines Facility-malaria, where the Global Fund negotiated bulk discounts from manufacturers and used both public and private sector for distribution,63 resulted in reduced manufacturer and end-user prices64 and rapidly increased the availability of artemisinin based combination treatments.64,65
Discussion
Countries have used different approaches to introduce task shifting when managing different diseases with notable improvements in efficiency and no adverse effects on patient care or outcomes. Similarly, investing in improved procurement and supply chain management have led to substantial efficiency gains and improved availability of medicines.
The evidence points to substantial opportunities for policymakers to promote better management of human resources and to strengthen procurement and supply chain management in order to improve health system efficiency and enhance health outcomes.
References
Grigoli F, Kapsoli J. Waste not, want not: the efficiency of health expenditure in emerging and developing economies. 2013.
Joshi R, Alim M, Kengne AP, et al. Task shifting for non-communicable disease management in low and middle income countries—a systematic review. PloS One. 2014;9(8):e103754.
Kredo T, Adeniyi FB, Bateganya M, Pienaar ED. Task shifting from doctors to non-doctors for initiation and maintenance of antiretroviral therapy. The Cochrane Database of Systematic Reviews. 2014;7:Cd007331.
Penazzato M, Davies MA, Apollo T, Negussie E, Ford N. Task shifting for the delivery of pediatric antiretroviral treatment: a systematic review. Journal of Acquired Immune Deficiency Syndromes (1999). 2014;65(4):414–422.
Polus S, Lewin S, Glenton C, Lerberg PM, Rehfuess E, Gulmezoglu AM. Optimizing the delivery of contraceptives in low- and middle-income countries through task shifting: a systematic review of effectiveness and safety. Reproductive Health. 2015;12:27.
Martinez-Gonzalez NA, Tandjung R, Djalali S, Rosemann T. The impact of physician-nurse task shifting in primary care on the course of disease: a systematic review. Human Resources for Health. 2015;13:55.
Committee on Understanding the Global Public Health Implications of Substandard F, and Counterfeit Medical Products; Board on Global Health; Institute of Medicine. Weaknesses in the Drug Distribution Chain. In: Buckley G, Gostin L, eds. Countering the Problem of Falsified and Substandard Drugs. Washington (DC): National Academies Press (US); 2013.
Munyaneza FH, Amoroso LR, Nyirazinyoye CL, et al. Leveraging community health worker system to map a mountainous rural district in low resource setting: a low-cost approach to expand use of geographic information systems for public health. Int J Health Geogr. 2014;13:49.
Datiko DG, Lindtjorn B. Cost and cost-effectiveness of smear-positive tuberculosis treatment by Health Extension Workers in Southern Ethiopia: a community randomized trial. PloS One. 2010;5(2):e9158.
Islam MA, Wakai S, Ishikawa N, Chowdhury AM, Vaughan JP. Cost-effectiveness of community health workers in tuberculosis control in Bangladesh. Bull World Health Organ. 2002;80(6):445–450.
Dick J, van Zyl M, Daniels K. Primary health care nurses implement and evaluate a community outreach approach to health care in the South African agricultural sector. Int Nurs Rev. 2007;54:383–390.
Okello D, Floyd K, Adatu F, Odeke R, Gargioni G. Cost and cost-effectiveness of community-based care for tuberculosis patients in rural Uganda. Int J Tuberc Lung Dis. 2003;7(9s1):S72–S79.
Clarke M, Dick J, Bogg L. Cost-effectiveness analysis of an alternative tuberculosis management strategy for permanent farm dwellers in South Africa amidst health service contraction. Scand J Public Health. 2006;34(1):83–91.
Khan MA, Witter JD, Imran SN, Safdar AN. Costs and cost-effectiveness of different DOT strategies for the treatment of tuberculosis in Pakistan. Health Policy Plan. 2002;17:178–186.
Prado TN, Guidoni LM, Golub JE, Dietze R, Maciel EL. Cost-effectiveness of community health worker versus home-based guardians for directly observed treatment of tuberculosis in Vitoria, Espirito Santo State, Brazil. Cad Saude Publica. 2011;27(5):944–952.
Alam K, Khan JA, Walker DG. Impact of dropout of female volunteer community health workers: an exploration in Dhaka urban slums. BMC Health Serv Res. 2012;12:260.
Yan H, Zhao J, Huan J, et al. The increased effectiveness of HIV preventive intervention among men who have sex with men and of follow-up care for people living with HIV after ‘task-shifting’ to community-based organizations: a ‘cash on service delivery’ model in China. PloS One. 2014;9(7):e103146.
Johns B, Ayalew E, Wong W, Bekele A, Kebede T, Palen J. Assessing the costs and effects of antiretroviral therapy task shifting from physicians to other health professionals in Ethiopia. J Acquir Immune Defic Syndr. 2014;65(4):e140–147.
Johns B, Baruwa E. The effects of decentralizing anti-retroviral services in Nigeria on costs and service utilization: two case studies. Health Policy Plan. 2016;31(2):182–191.
Fatti G, Monteith L, Shaikh N, Kapp E, Foster N, Grimwood A. A comparison of two task-shifting models of pharmaceutical care in antiretroviral treatment programs in South Africa. J Acquir Immune Defic Syndr. 2016;71:e107–113.
Babigumira JB, Castelnuovo B, Stergachis A, Kiragga A, et al. Cost effectiveness of a pharmacy-only refill program in a large urban HIV/AIDS clinic in Uganda. PloS One. 2011;6(3):e18193.
Foster N, McIntyre D. Economic evaluation of task-shifting approaches to the dispensing of anti-retroviral therapy. Human Resources for Health. 2012;10:32.
Ruebush TK, Zeissig R, Koplan JP, Klein RE, Godoy HA. Community participation in malaria surveillance and treatment. III. An evaluation of modifications in the Volunteer Collaborator Network of Guatemala. Am J Trop Med Hyg. 1994;50(1):85–98.
Sikaala CH, Chanda C, Hamainza J, et al. A cost-effective, community-based, mosquito-trapping scheme that captures spatial and temporal heterogeneities of malaria transmission in rural Zambia. Malar J. 2014;13:225.
Jafar TH, Islam M, Bux R, Poulter N, Bergström S. Cost-effectiveness of community-based strategies for blood pressure control in a low-income developing country: findings from a cluster-randomized, factorial-controlled trial. Circulation. 2011;124(15):1615–1625.
Puett C, Sadler K, Alderman H, Coates J, Fiedler JL, Myatt M. Cost-effectiveness of the community-based management of severe acute malnutrition by community health workers in southern Bangladesh. Health Policy Plan. 2013;28(4):386–399.
Laveissiere C, Meda A, Doua F, Sane B. Detecting sleeping sickness: comparative efficacy of mobile teams and community health workers. Bull World Health Organ. 1998;76(6):559–564.
Buttorff C, Hock RS, Weiss HA, Naik S, et al. Economic evaluation of a task-shifting intervention for common mental disorders in India. Bull World Health Organ. 2012;90(11):813–821.
Kruk ME, Pereira C, Vaz F, Bergström S, Galea S. Economic evaluation of surgically trained assistant medical officers in performing major obstetric surgery in Mozambique. BJOG. 2007;114(10):1253–1260.
Sadruddin S, Bari S, Khan A, Qazi S. Household costs for treatment of severe pneumonia in Pakistan. Am J Trop Med Hyg. 2012;87(5 Suppl):137–143.
Chuit R, Paulone I, Wisnivesky-Colli C, Bo R, Perez A, Sosa-Stani S, Segura EL. Result of a first step toward community-based surveillance of transmission of Chagas’ disease with appropriate technology in rural areas. Am J Trop Med Hyg. 1992;46(4):444–450.
Homedes N, Ugalde A. Improving access to pharmaceuticals in Brazil and Argentina. Health Policy Plan. 2006;21(2):123–131.
Chaudhury RR, Parameswar R, Gupta U, Sharma S, Tekur U, Bapna JS. Quality medicines for the poor: experience of the Delhi programme on rational use of drugs. Health Policy Plan. 2005;20:124–136.
Li Y, Ying C, Sufang G, Brant P, Bin L, Hipgrave D. Evaluation, in three provinces, of the introduction and impact of China’s National Essential Medicines Scheme. Bull World Health Organ. 2013;91(3):184–194.
Khoja TA, Bawazir SA. Group purchasing of pharmaceuticals and medical supplies by the Gulf Cooperation Council states. East Mediterr Health J. 2005;11(1–2):217–225.
Al-Abbadi I, Qawwas A, Jaafreh M, Abosamen T, Saket M. One-year assessment of joint procurement of pharmaceuticals in the public health sector in Jordan. Clin Ther. 2009;31(6):1335–1344.
Amaral S, Blatt CR. Municipal consortia for medicine procurement: impact on the stock-out and budget. Rev Saude Publica. 2011;45(4):799–801.
Milovanovic DR, Pavlovic R, Folic M, Jankovic SM. Public drug procurement: the lessons from a drug tender in a teaching hospital of a transition country. Eur J Clin Pharmacol. 2004;60(3):149–153.
Sigulem F, Zucchi P. E-procurement in the Brazilian healthcare system: the impact of joint drug purchases by a hospital network. Pan Am J Public Health. 2009;26(5):429–434.
Adesina A, Wirtz VJ, Dratler S. Reforming antiretroviral price negotiations and public procurement: the Mexican experience. Health Policy Plan. 2013;28(1):1–10.
Chaumont C, Bautista-Arredondo S, Calva JJ, et al. Antiretroviral purchasing and prescription practices in Mexico: constraints, challenges and opportunities. Salud Publica Mex. 2015;57 Suppl 2:s171–182.
Tren R, Bate R. Drug procurement, the Global Fund and misguided competition policies. Malar J. 2009;8:305.
Ewen M, Al Sakit M, Saadeh R, et al. Comparative assessment of medicine procurement prices in the United Nations Relief and Works Agency for Palestine Refugees in the Near East (UNRWA). J Pharm Policy Pract. 2014;7(1):13.
Bukhari S, Qazi J, Jooma R, Bile K, Kazi G, Zaibi W, Zafar A. Essential medicines management during emergencies in Pakistan. East Mediterr Health J. 2010;16 Suppl:S106–113.
Berger EJ, Sauveur D, Manasse M, et al. Implementation and evaluation of a web-based system for pharmacy stock management in rural Haiti. AMIA Symposium. 2007:46–50.
Shieshia M, Andersson M, Felling S, et al. Strengthening community health supply chain performance through an integrated approach: Using mHealth technology and multilevel teams in Malawi. J Glob Health. 2014;4(2):020406.
Mikkelsen-Lopez I, Cieza A, Kasale H, Mbuya C, Reid G, de Savigny D. Essential medicines in Tanzania: does the new delivery system improve supply and accountability? Health Syst (Lond). 2014;3(1):74–81.
Daff BM, Seck C, Belkhayat H, Sutton P. Informed push distribution of contraceptives in Senegal reduces stockouts and improves quality of family planning services. Glob Health Sci Pract. 2014;2(2):245–252.
Steyn F, Engelbrecht M, van Rensburg-Bonthuyzen EJ, Jacobs N, van Rensburg DH. Scaling up access to antiretroviral drugs in a middle-income country: public sector drug delivery in the Free State, South Africa. AIDS Care. 2009;21(1):1–6.
Lloyd J, McCarney S, Ouhichi R, Lydon P, Zaffran M. Optimizing energy for a “green” vaccine supply chain. Vaccine. 2015;33(7):908–913.
Riewpaiboon A, Sooksriwong C, Chaiyakunapruk N, et al. Optimizing national immunization program supply chain management in Thailand: an economic analysis. Public Health. 2015;129(7):899–906.
Witter S. Achieving sustainability, quality and access: lessons from the world’s largest revolving drug fund in Khartoum. East Mediterr Health J. 2007;13(6):1476–1485.
Knippenberg R, Alihonou E, Soucat A, et al. Implementation of the Bamako Initiative: strategies in Benin and Guinea. Int J Health Plann Manage. 1997;12 Suppl 1:S29–47.
Uzochukwu BS, Onwujekwe OE, Akpala CO. Effect of the Bamako-Initiative drug revolving fund on availability and rational use of essential drugs in primary health care facilities in south-east Nigeria. Health Policy Plan. 2002;17(4):378–383.
Tougher S, Ye Y, Amuasi JH, et al. Effect of the Affordable Medicines Facility-malaria (AMFm) on the availability, price, and market share of quality-assured artemisinin-based combination therapies in seven countries: a before-and-after analysis of outlet survey data. Lancet. 2012;380(9857):1916–1926.
Sabot OJ, Cohen A, Mipuge J. Piloting the global subsidy: the impact of subsidized artemisinin-based combination therapies distributed through private drug shops in rural Tanzania. PloS One. 2009;4(9):e6857.
Gabriel Seidman, DrPH Candidate, Harvard T.H. Chan School of Public Health
Dr. Rifat Atun, Professor of Global Health Systems, Harvard T.H. Chan School of Public Health
Chilean President Michelle Bachelet arrived in her office in Santiago early on Monday morning. She was preparing for her afternoon meeting with the Presidential Advisory Commission and senior colleagues at the Ministry of Health and the Ministry of Finance.
To-date, Chile has two separate and unequal health care financing and provision systems, established by the Pinochet regime in the 1970s and 80s. President Michelle Bachelet, who took office in March 2014, convened a Presidential Advisory Commission to propose how to resolve the divide between the two sub-systems of public and private healthcare financing and delivery that have been in place in Chile for the last 30 years. The previous Presidential Commissions formed prior to 2014 were unable to find consensus on a health reform for the country. President Bachelet hopes to lead a health sector reform as part of her Presidential legacy.
As President Bachelet prepared for her afternoon meeting, she decided to review some historical facts about the health sector in Chile one more time, as well as the advantages and disadvantages of the public-private partnership in financing health care. Lastly, she is considering the two alternative health reforms voted for by the Presidential Commission.
What would you consider as the advantages and disadvantages of the Chilean model? What lessons do you learn for guiding your decisions about public and private partnership in financing healthcare?
Introduction
Chile, a high-income country in South America, has a population of 17 million people who enjoy an average GDP per person of $21,030 (ppp int $) (2014). Chile’s income is unequally distributed with a high Gini Coefficient of 0.51 in 2011 (1) with the average income of the richest quintile being 17.5 times higher than that of the poorest quintile and the richest 20 percent earning 58 percent of GDP (2). Chile has an under-five mortality rate of 8 per 1,000 live births and a maternal mortality rate of 22 (2013), health outcomes better than the average of upper middle income Latin American nations. Its national Total Health Expenditure (THE) was 7.4 percent of GDP in 2013 with 54 percent coming from private sources (3).
In the 1950s, the Chilean democratic Government established a national health service similar to the UK’s National Health System (NHS) model. The Government budget funded public health services to assure every citizen had basic health services. The Chilean health care system emphasized prevention and treatment of communicable diseases and maternal and child health services (4). However, the underfunding of this public scheme in addition to the rigid bureaucratic management of public health services resulted in long waiting times, inefficiency and poor quality of services. The Pinochet regime, an authoritarian military regime which took over the Chilean Government in 1973, decided to address the existing problems via a market approach for public and private health insurance. The Pinochet regime shared an ideology with the Chicago boys, a group of Latin American economists who studied or identified with neoliberal economic theories taught at the University of Chicago and advocated for a small Government, individual choice, private property and ownership, private market and minimum taxes.
1 The case was prepared under the guidance of William Hsiao. Cristian A. Herrera provided some of the data and prepared the first draft, Maria Joachim wrote the case and Ricardo Bitran reviewed and commented on the case.
As a result, the military regime continued to provide universal free primary health care with Government financing but it turned to a two-tiered approach for ambulatory and hospital services, thus giving rise to two different subsystems for health financing. Chile today relies on social health insurance (SHI) with two plans, the public plan (FONASA) covering about 78 percent of the population and private insurance plan (ISAPREs) covering about 17 percent of the population to provide nearly universal health coverage to its 17 million people (5).
Historical Development
The National Health Fund and the Private Health Prevision Institutions (1979 – 1990)
As a result of the ideologies of the Pinochet regime, Chile has had two public and private subsystems for over 30 years. As designed by the Pinochet regime, the public subsystem consisted of the large public insurer known as FONASA (Fondo Nacional de Salud, or National Health Fund). FONASA insured the majority of the Chilean population, including the indigent, low- and middle-income citizens and retirees. It covered primary and hospital health care delivered mostly through public providers while also offering a voucher system to subsidize general and specialty ambulatory care with private providers. The Government at the time also tried to improve the quality of public services by decentralizing Primary Health Centers (PHCs) from the central Government to municipalities. Financing for PHC was provided mostly by the central Government but municipalities were encouraged to contribute more, thus enhancing financing contributions to improve the quality of care for the Chilean population.
Despite decentralization to improve efficiency and quality, the Chilean public health services were still characterized by low levels of efficiency and quality. At the time, the Government also considered the introduction of modern management tools for public hospitals but little was done to implement such reforms. Hospital health workers’ unions were politically strong and opposed hospital management reforms. Given the political ideology of the Pinochet regime, which advocated deregulation and privatization, several insurers known as ISAPREs (Instituciones de Salud Previsional, or Health Prevision Institutions), were chosen as the alternative financing option to the public FONASA. ISAPREs, established in 1981, were for-profit private insurers that covered a small minority of the more affluent population (about 5 percent of the Chilean population) and provided services almost exclusively in the private sector (5). It is worth noting that in the 2000s, the Government attempted to suggest public management reform for the public sub-system once more but again, without much success.
In 1979, when the Pinochet regime decided to establish private insurance financing, the public FONASA was funded by a 4 percent of wages from formal sector workers in order to supplement the national Government’s health budget to pay for services provided by public health providers. In 1981, a parallel private insurance market was set up by allowing this tax of 4 percent to be transferred to the private ISAPREs. The first impact of the ISAPREs on public health services was the migration of higher income employees to ISAPREs. After the creation of the ISAPREs, hundreds of individuals started opting out of the public FONASA and directing their mandatory 4 percent health tax to ISAPREs. That movement created a financing gap for FONASA which had to be covered by the Ministry of Finance. To achieve universal coverage, Chile requires, by law, that all formal sector workers enrol in either FONASA or ISAPREs. ISAPREs have been allowed to charge an additional premium to their affiliates on the basis of an individually health risk condition and coverage of catastrophic health expenses. It should be highlighted that Chile gives individuals a choice for health insurance enrollment; those who are able and willing to pay the additional ISAPREs premiums can opt out of the public FONASA. At its inception, the Government provided an additional subsidy equal to 2 percent of the salary to those workers who wanted to join an ISAPRE so they can obtain the type of benefits they want. Other individuals, such as informal sector workers may choose to buy insurance from ISAPREs or FONASA. FONASA accepts any person regardless of their employment status or income. Unemployed and indigent individuals have the right to free coverage by FONASA.
The second impact of ISAPREs has been the more recent phenomenon of migration of physicians to the private sector (see below).
While the mandatory payroll health tax was set initially at 4 percent, ISAPREs pushed for an increase and after a few years, the contribution was increased to 7 percent, a percentage (up to a monthly salary ceiling of US$2,700), which still holds valid today for both FONASA and ISAPREs. The Government transfers the 7 percent payroll tax to ISAPREs for affiliates who enrol in it. In addition to the 7 percent contribution required by all FONASA and ISAPREs beneficiaries, ISAPREs, on average, charges an extra 3 percent of wages as additional premium to cover other benefits such as individual health risk, and catastrophic coverage. Catastrophic expenses under FONASA are covered in the standard contribution of 7 percent.
With regards to benefit packages, FONASA beneficiaries have had to make small copayments for ambulatory and inpatient services provided in public hospitals while ISAPRE beneficiaries have been required to make higher co-payments in public hospitals (6). FONASA covers and fully subsidizes indigent families. FONASA has also implemented a voucher system to cover a part of the cost of private care for its non-indigent beneficiaries. ISAPREs purchases most health services from private providers that are allowed to freely open facilities with only some minor sanitary regulations.
The Current Structure (1990s – present)
Chile returned to democracy in 1990 after a plebiscite that voted out Pinochet’s military regime. The new Governments were inspired by Christian humanism and social democrat ideas, pushing for reforms to correct the previous inequitable policies and weak regulation of the private sector. First, the State eliminated the additional 2 percent subsidies for enrollment in ISAPREs. Second, the Superintendence of ISAPREs was created to regulate the private insurance and the private provider markets. Third, in the early 2000s, the Government advocated for a significant health reform that created the Regime of Explicit Guaranties in Health known as AUGE (Acceso Universal con Garantias Explicitas), covering preventive and curative services for 80 prioritized health conditions (representing around 80 percent of the health burden). AUGE mandated SHI insurers to adopt the package via explicit legal guarantees for all beneficiaries as a tool to break the divide in the two-tiered health system. The AUGE law now governs the entire Chilean SHI system and applies to the indigent and the nonindigent members of FONASA as well as the higher-income beneficiaries of ISAPREs. The AUGE package guarantees not only treatments, but also sets upper limits on waiting times and Out-Of-Pocket (OOP) payments for treatments (7).
The Public-Private Health Financing Scheme: Advantages and Disadvantages
Advantages of Private Insurers in the Health Financing Scheme
Shared Government Budget
The FONASA per capita expenditure includes the 7 percent mandatory health contribution plus public subsidies that Government makes to FONASA which currently represents about two-thirds of FONASA’s budget. Real expenditure per capita for FONASA enrollees has increased from US$300 (2002) to US$508 (2011). The ISAPREs per capita expenditure figures include both the 7 percent mandatory health contribution and the additional voluntary contribution which averages another 3 percent points. Real expenditure per capita for ISAPREs enrollees has increased from US$720 (2002) to US$832 (2011). While ISAPREs’ per capita spending remains higher than FONASA’s, the gap between the two has been decreasing over time (5). It is worth noting that ISAPREs reached their peak coverage in 1995, covering about 26 percent of the population. Since then, ISAPREs coverage dropped; this can be explained by improvements in FONASA and the AUGE reforms which have been making FONASA a relatively more attractive option for the Chilean population.
The Chilean Government has been spenting a larger share of its budget for health, growing from 12.2 percent in 2000 to 13.9 percent in 2011. The AUGE reform has been accompanied by a sizable increase in total health spending in the country, both from public and private sources. In absolute, real terms, THE per capita has grown by 48 percent, from 2000 to 2011. Nevertheless, with the rapid economic growth, The Total Health Expenditure (THE) of Chile has fallen as a share of GDP from 8.4 percent in 2000 to 7.3 percent in 2011. It is worth noting that despite insurance coverage from both FONASA and ISAPREs, the large source of health financing for Chile is OOP spending. OOP spending amounts to to 38.2 percent of THE (7).
Source: Bitran R. 2013. UNICO Studies Series 21 Explicit Health Guarantees for Chileans: The AUGE Benefits Package. The World Bank, Washington DC (7).
User Satisfaction with Services and Perception of Protection
No systematic evaluation of health outcomes is available for FONASA and ISAPREs. However, we present a comparison of patients’ rating of their satisfaction with FONASA and ISAPREs on a few dimensions where data is available. There is no data on the difference in their clinical quality (8).
Source: Table constructed by case authors based on information provided in: Estudio de opinión a usuarios del sistema de salud, reforma y posicionamiento de la Superintendencia de Salud. Enero 2014, Superintendencia de Salud (8).
• Infrastructure, Technologies and Human Resources Investment
An impact of ISAPREs has been the more recent phenomenon of migration of physicians to the private sector, where they have better working opportunities and higher incomes. The Government has responded to this challenge by increasing the salaries of public physicians but to a level that is still less tan the private sector. The Government has also removed the requirement of having to pass a national medical board test to practice medicine in order to attract foreign physicians from Ecuador, Spain, Cuba, Spain, and other countries into the public health care system.
Furthermore, ISAPREs have been instrumental in boosting private investment for health. There is almost no regulation on private providers investing in new medical technology. Competition between public and private providers propelled new investments in the major cities for new private hospitals and accelerated the introduction of new medical technologies. By 2012, private sector owned 22.4 percent of hospital beds in Chile with an increase of 24 percent of private for-profit beds between 2005 and 2012 (9).
Catastrophic Expenditure Coverage
By regulation, every ISAPRE plan must include coverage for catastrophic diseases (known as CAEC by its Spanish acronym) in its benefit package, funded by the 3 percent additional premium. CAEC requires the beneficiaries to pay a deductible of US$4,800 for each disease suffered. FONASA also covers the catastrophic expenses, but without charging additional premium. Despite the establishment of CAEC, patient financial protection is a concern for beneficiaries of both FONASA and ISAPREs. While the establishment of CAEC provides additional financial protection, Bitran and Munoz have shown that the incidence of catastrophic expenditure for Chilean households does not depend on income or insurance schemes, indicating that neither FONASA nor ISAPREs adequately addresses the problem of providing financial protection against catastrophic health expenditures (10).
It is worth nothing that 25 percent of patients covered by ISAPRES receive services in public facilities because they cannot afford the ISAPREs co-payments (11, 12) while almost half of all catastrophic events among children of ISAPRES members are treated in public hospitals (13).
In recent years, comercial insurance to cover catastraphic expenses has grown rapidly, purchased by 4.6 million people. The majority of the purchasers are reported to be the middle- and upper-income individuals covered by an ISAPRE who seek further financial protection through private insurance (7).
Disadvantages of Having Private Insurers in the Chilean Health Financing Scheme
Disparity by Income and Risk Selection
First, the public-private insurance system is segmented by income, with the majority of low-and middle-income groups enrolled in the public FONASA; 79 percent of the population is covered by the public system. There is neither risk pooling nor income re-distribution between the sub-systems—FONASA and ISAPREs—thus segregating the rich and the poor. As the ISAPREs affiliates also pay premiums on top of the mandatory 7 percent of their wages (thus a total of about 10 percent of their wages), ISAPREs receive 54 percent of all the total revenues for the social insurance schemes to provide coverage only to 16.5 percent of the Chilean population (14).
Second, ISAPREs segment their market by charging an additional premium according to individual health risks. To assess the individual risk, ISAPREs attempt to predict the future health expenditure for each person and charge the premium accordingly. Consequently, less healthy people and women in childbearing age have to pay significantly higher premiums to buy or continue enroll in an ISAPRE plan. As a result, the great majority of the less healthy people are covered by FONASA. In addition, the proportion of people over 60 years is significantly higher in FONASA than in ISAPREs.
Third, the pre-existence of diseases constitutes a major challenge for ISAPREs beneficiaries. Those with pre-existing conditions or for reasons of age or gender have a limited ability to shift its enrollment to another ISAPRE plan. As a result, 39 percent of all ISAPREs affiliates are ‘captive’ because if they change to another ISAPRE, they might not be able to afford the new required premium (14). Furthermore, the pre-existence of diseases does not allow affiliates with chronic conditions to switch from FONASA to any ISAPREs plan as they wish. The Government is not willing to compensate ISAPREs for the actuarial risk of FONASA beneficiaries that decide to migrate to an ISAPRE.
Imperfect Insurer-Provider Relationship in the Private Sector
First, vast majority of the private services were paid by fee-for-service (FFS). Under FFS, providers induce demand so they can earn higher income and jeopardizes cost containment and efficiency. Moreover, the fees paid by ISAPREs to private providers are defined on a free market basis, separately from the public sector, where standard Government-defined tariffs are listed for all services provided by public facilities. Consequently, payment rates are much higher in the private sector. In addition more resources and better infrastructure are available in the private sector, therefore attracting physicians and nurses with higher wages and leaving the public sector understaffed.
Increasing Number of Judicial Accusations Against ISAPREs
ISAPREs have witnessed an exponential growth in the number of lawsuits from their affiliates due to changes in premium prices. 60 percent of the cases processed by the Appellation Courts are related with ISAPREs (14, 15).
Deregulation of Complementary and Supplementary Insurance
ISAPREs can be considered as both complementary (covering services beyond the basic coverage offered by FONASA) and supplementary (covering some services that are not included in FONASA’s basic coverage). ISAPREs are able to provide these plans because they get the mandatory contribution and extra premiums, thus collecting about 10 percent of the richest wages in Chile.
Current Health Financing Reform Options under Discussion in Chile
The current health system in Chile requires reform: risks are not pooled, members are charged premiums according to their health conditions and are unable to switch between ISAPREs because of pre-existing conditions while the private insurers issue their own rules and set their annual premiums without transparency. After President Michelle Bachelet took office in March 2014, she convened the Third Presidential Advisory Commission for Health Reform. Along with her leadership, the delegation of Commissioners voted on medium- and long-term health reform alternatives: a National Health Insurance System and a Social Health Insurance. Similar to the First and Second Commissions, the Third Commission under Bachelet’s leadership did not deliver a consensus report but contrary to the two previous Commissions, it did achieve majority and minority views for health financing reform.
The Minority View: Social Health Insurance System (SHI)
The minority view supports keeping the two-tiered health system now in place but solving some of the aforementioned problems of ISAPREs. Under the SHI model, collection of financial resources relies on the labor market; payroll taxes can be deducted from worker’s wages and companies’ taxes with State subsidies as contributions.
The “minority” position is to preserve the current system of competition among insurers but to solve the problem of captivity in ISAPREs by setting up a Risk Equalization Fund (REF) fund among them as a means to adjust risk and make it illegal for ISAPREs to reject clients based on age, gender and health status. In addition, the minority position seeks to make ISAPRE plans more transparent and to require all ISAPREs to offer the same benefits package, known as Guaranteed Health Plan (GHP), while allowing them to sell complementary insurance above the GHP. The contents of the GHP would largely exceed the contents of AUGE. In fact, the GHP would contain AUGE, plus catastrophic coverage, plus coverage for preventive care, plus coverage for all non-AUGE services (7). Further, each ISAPRE would offer this plan at a single price for all beneficiaries irrespective of their age, gender, or health status.
The Majority View: National Health Insurance System (NHI)
The majority view supports a single payer, single public insurer instead of keeping the SHI currently in place. In this alternative, collection of funds would be the same as for SHI, with contributions from workers, enterprises and the State. In addition, the resources collected would be pooled in a single fund that would be managed by a public autonomous entity.
The main difference between the two suggested models would be on the purchasing side. The NHI model would be a public single-payer system that would purchase services for the entire population, based on a single benefit package guaranteed for all. The management of the single-payer would have a participatory board with representation of public and private actors (including users) related with the system. On the side of providers, the existence of public and private facilities would be maintained, but the Government would regulate the contractual relations and payment rates, thus stimulating more coordinated networks of care. Co-payments would be regulated and made homogeneous and proportional to the income of the affiliate and with a stop-loss mechanism to avoid impoverishment due to health expenditures. Through this scheme, ISAPREs could be transformed into complementary and/or supplementary health insurers that would be supervised by the Superintendence of Health.
Molina C. 2006. “Antecedentes del Servicio Nacional de Salud. Historia de Debates y Contradicciones. Chile: 1932-1952.” Cuadernos Médico Sociales (Chile), 46(4): 284-304.
Bitran R. April 21, 2015. “The Public-Private Health Financing System in Chile: Winds of Reform.” Ministerial Leadership In Health. Harvard T.H. Chan School of Public Health.
Jimenez J & Bossert T. 1995. “Chile’s health sector reform: lessons from four reform periods.” Health Policy, 32: 155-166.
Bitran R. 2013. UNICO Studies Series 21. “Explicit Health Guarantees for Chileans: The AUGE Benefits Package.” The World Bank, Washington DC.
Superintendencia de Salud. Enero 2014. Estudio de opinión a usuarios del sistema de salud, reforma y posicionamiento de la Superintendencia de Salud.
Asociación de Clínicas de Chile. Diciembre 2013. “Dimensionamiento del sector de salud privado en Chile. Actualización a cifras del año 2012.”
Bitran R, Muñoz R. 2012. “Chapter 6: Health Financing and Household Health Expenditure in Chile”, in Knaul FM, Wong R, Arreola-Ornelas H. “Household Spending and Impoverishment.” Volume 1 of Financing Health in Latin America Series. Cambridge, MA: Harvard Global Equity Initiative, in collaboration with Mexican Health Foundation and International Development Research Centre, 2012; distributed by Harvard University Press. Available at: http://www.idrc.ca/EN/Documents/Financing-Health-in-Latin-America-Volume-1.pdf
Annick M. 2002. “The Chilean health system: 20 years of reforms.” Salud Publica Mex 44: 60–68.
Larrañaga O. 1997. “Eficiencia y equidad en el sistema de salud chileno.” CEPAL 49: 1–45.
World Bank. 2000. “Chile health insurance issues: old age and catastrophic health costs.”
Comisión Asesora Presidencial para el Estudio y Propuesta de un Nuevo Marco Jurídico para el Sistema Privado de Salud. Informe Estudio y Propuesta de un Nuevo Marco Jurídico para el Sistema Privado de Salud. October 8th 2014. Available at: http://web.minsal.cl/comision_asesora_presidencial. Accessed on March 14th 2015.
Policymakers can use investments in health and health systems to create value in two distinct but related ways: by generating “value for money” and “value for many”.1 Value for money refers to the relative magnitude of a positive output or outcome relative to the size of investment, typically measured using cost effectiveness tools, whereas value for many refers to the distribution and equity of the outcome among the population. Thus, government officials must carefully consider how to prioritize budgets in order to generate the most value, defined broadly, in their country.
The total size and allocation of a budget for health expenditures can have direct and indirect impacts on population health.2,3 Indeed, low- and middle-income countries (LMICs) with similar Gross Domestic Product (GDP) levels, similar health expenditures as a proportion of GDP, and similar per person expenditure levels on health have highly varying health outcomes on a number of dimensions, including life expectancy, infant mortality, maternal mortality, and availability of treatment for diseases such as HIV and diabetes.4
In addition, investing in health also brings distinct economic benefits for the country5–10 and political benefits for the policymakers who choose to prioritize health. Microeconomic evidence suggests that healthy development of children allows for increased income later in life and general health of adults has positive impacts on their income. At the macroeconomic level, health of the population can lead to growth in the country’s economy through increased labor productivity, increased incentives for individuals to invest their incomes due to longer life expectancy, and a “demographic dividend.” With regards to the political implications of allocating resources for health, health is a major concern among the public in countries of all income levels, including low-income countries.11 Cases from Turkey, Brazil, and the UK demonstrate that government prioritization of health investments can have a positive impact for governing parties that commit to investing in and strengthening health systems.
This document provides an overview of four key questions that policymakers can consider when determining how to generate the most value through health budget priority-setting:
What values underlie the government’s priorities for the country?
Based on these values, what goals for the healthcare system does the government hope to achieve?
Based on these goals, where should the government allocate its financial resources for health?
How should the government allocate its financial resources for health?
We will first address these questions and then consider the potential health, economic, and political consequences of various health budget allocation decisions.
What Values Underlie the Government’s Priorities for the Country?
Although a broad range of values can drive the government’s approach to resource allocation, these value sets generally fall into three broad categories: utilitarian, liberal, and communitarian.5
Utilitarians are consequentialists and focus on the value, or utility, that a policy or other decision will have. Using a consequence-based approach to decision-making, utilitarians generally believe “the ends justify the means” (assuming “the means” involve ethical and legal decisions). Policy analysis tools such as cost-effectiveness and cost-benefit analysis reflect utilitarian concerns of generating the greatest outcome for the greatest number of people using the fewest possible resources. Of course, predictive uncertainty about the total utility that a policy will generate causes difficulty for utilitarians. Further, utilitarians differ in how they would choose to measure total utility. Subjective utilitarians argue that value is subjective to the individual and that individuals must judge their own happiness for themselves. Accordingly, subjective utilitarians might measure the total utility of a product or service using the price that a person would willingly pay for it. In contrast, objective utilitarians argue that individual’s choices are not always rational or valid and that an objective index of well-being is better suited to measure utility. Such indices include Disability-Adjusted Life Years (DALYs) and Quality-Adjusted Life Years (QALYs), which are composite indices combining number of years lived as a result of an intervention (adjusted for disability or quality of those years lived); health economists employ these measures in cost effectiveness analyses in order to compare and argue for certain policies over others. Some might describe pure utilitarianism as “ruthless” in that it can justify excluding certain populations who would cost too much to treat (e.g. rural populations without easy access to a medical facility). Hence, equity is not the primary concern of utilitarians, who are more likely to prioritize efficiency and effectiveness.
Liberals take a rights-based approach to allocation of health resources. Liberals believe that all humans have the capacity and obligation to display mutual respect to each other, and this mutual respect endows individuals with rights, or “claims that all individuals can make on each other by virtue of their humanity.” Some liberals, known as libertarians, focus only on negative rights, which guarantee individual freedom. For example, libertarians might focus on the rights of the individual to choose their physician. In contrast, egalitarian liberals also emphasize the importance of positive rights, or a minimum level of resources and services, which can guarantee the ability for an individual to exercise his or her free choices. Accordingly, egalitarian liberals tend to favor redistribution of resources in order to ensure that the entire population has access to basic positive rights. However, with regards to prioritizing health, egalitarian liberals differ in their views on whether individuals have a right to health services (i.e. provision of and access to care) or health status (i.e. the achievement of general well-being).
In contrast to the first two value sets described, communitarians do not focus on the level of the individual in assessing a policy, but rather on the level of the community or society; in other words, they recognize the social nature of life in their assessment of policies. As such, communitarians evaluate the merit of a policy on whether it adheres to a community’s value set and whether it promotes individuals and a society consistent with that value set. Thus, communitarians would generally oppose a health policy which achieved positive population health outcomes with an intervention that defied local cultural norms or values. Communitarians fall into two broad categories: those who believe in a single set of values which would promote a better society (universal communitarians), and those who argue that each society should set its own values and norms based on the context-specific factors (relativist communitarians).
Before moving on to discuss how values could lead to different goals for the healthcare system, one should note that these value sets are not necessarily mutually exclusive. Policymakers might include both a utilitarian and communitarian perspective in an analysis where they prioritize health interventions based on their objective utility, but choose to exclude any that overtly defy local norms. Further, governments can modify their ethical values as they learn more about a population’s needs and their ability to meet those needs. However, it is important to maintain adequate “coherence and explicitness” when articulating one’s values; doing so creates transparency for the population and gives others the opportunity to agree with the government’s choices because they can understand the rationale behind these choices.
Based on These Values, What Goals for the Healthcare System Does the Government Hope to Achieve?
Policymakers must consider which outputs and outcomes to prioritize when allocating resources for health investments. In this context, the term outputs refers to how well the health system performs its delivery of personal and public health services to the population, whereas outcomes, also known as goals, refer to the ultimate ends that the health system aims to achieve. These goals include health status, financial protection, and user satisfaction. (See Figure 1 for an overview of a health system’s functions, objectives, outputs, and outcomes.) In many cases, strong delivery of health systems outputs is necessary but not sufficient for strong performance on health systems outcomes. Below we discuss how a policymaker might prioritize health systems outputs and outcomes, and how the three value sets described above might influence the balance of objectives a policy maker might have in relation to health system outputs and outcomes.
A policymaker needs to balance four key objectives for the outputs achieved by a health system: equity, efficiency, effectiveness, and responsiveness.12 The four objectives for health systems outputs are:
Equity refers to the differences in how a policy affects people of different groups. The most common concern is equity among populations of different income groups in relation to access to health system outputs or in relation to health outcomes. Other equity issues, such as disparities between rural and urban populations, also should and often do inform policy. An analysis of a policy’s “vertical equity” takes into account its differential impact across populations at different income levels, whereas an analysis of “horizontal equity” looks at whether the policy treats individuals at the same income level the same.5
Efficiency has been defined many ways in the fields of policy analysis. For the purposes of health systems analysis, we define efficiency using the concept of technical efficiency, drawn from economics. Technical efficiency accounts for whether society is producing the most goods and services for the least cost.
Effectiveness refers to whether interventions are evidence-based and safe.12 In other words, an effective intervention will achieve the desired health outcomes.
Responsiveness refers to whether the health system meets the public’s legitimate nonmedical expectations. Responsiveness is a highly subjective measure and depends on the perceptions among citizens of a health system’s functioning.13
Without a doubt, policymakers’ values will influence which health system objectives they choose to prioritize for the health system outputs. For example, pure utilitarians will likely care most about efficiency and effectiveness, and they will less likely prioritize equity. They might also disregard the importance of responsiveness as an objective, unless they believe that a health system’s responsiveness generates value for the population. Liberals, who focus on individuals’ rights, will prioritize equity and responsiveness of the system, with libertarians emphasizing the importance of choice and egalitarian liberals emphasizing the equity in access to positive rights (e.g. basic health services and medicines). Communitarians, who emphasize society’s values, will prioritize the objectives most relevant for achieving the best possible society. Accordingly, they will likely emphasize responsiveness and equity of the system at a societal level.
In addition to setting objectives for health systems outputs, policymakers must also pay attention to the health systems outcomes, or the overall goals for a country’s health system. These fall broadly into three categories: population health status, financial risk protection, and citizen satisfaction.5,12
Health status refers to the actual health of a population. Measurements of population health status include life expectancy, burden of disease, mortality rates for specific groups (e.g. infant mortality and maternal mortality), and prevalence of specific diseases.
Financial risk protection refers to helping people avoid very large and unpredictable payments for health, sometimes known as catastrophic expenditures. Mechanisms to provide financial risk protection typically involve insurance schemes with risk-pooling functions. Measuring levels of financial risk protection can be difficult because a person having insurance coverage does not necessarily mean that they have coverage for a complete package of basic medicines and services. In addition, individuals may technically have insurance to cover medicines and services, but they may not actually have access to these services (e.g. due to geographic disparities, physician shortages, or drug stockouts), thereby rendering their insurance coverage of little value.
Citizen satisfaction refers to the degree with which users of the health system rate the system as satisfactory. Citizen dissatisfaction with the health system can serve as a major catalyst for reform, as we will discuss later. Measuring citizen satisfaction typically involves conducting surveys with citizens and possibly evaluating their willingness to pay for services.
As with health systems outputs, health systems outcomes also derive directly from the value sets described earlier. For example, objective utilitarians might concern themselves most with the population’s average health status, whereas egalitarian liberals might focus most on the range of health status (as a measure of equity levels). Egalitarian liberals will also emphasize the importance of financial risk protection as a means for ensuring minimum economic opportunities for all. Subjective utilitarians might place a high value on citizen satisfaction, as would libertarians (in the sense that satisfaction relates to an individual’s level of choice.)
Based on These Goals, Where Should the Government Allocate Its Financial Resources for Health?
Once the government has identified its objectives for the outputs and outcomes of the health system, it can decide upon specific programs or interventions to achieve these goals and allocate budgets accordingly. In this section, we describe the decisions a government faces about where to allocate its resources. In the next section, we describe a process and framework for making these allocation decisions.
As shown in Figure 1, a health system has four main functions which a government can prioritize for investment to develop a well-functioning health system: governance and organization, health financing, resource management, and healthcare / public health services. Governments can also choose to invest in specific disease programmes or interventions, as discussed below.12
Governance and organization encompasses the organizations and institutions involved in delivering products and services to citizens.14 The organization of the health system includes hospitals, primary care clinics, and supply chains which provide medicines to providers. A government could choose to invest in the governance and organization of the health system, for example, by updating management policies for health facilities, changing the referral network of the system, or improving processes for decision-making at the programmatic level.
Health financing involves the provision of insurance plans to offer financial risk protection to citizens. Mechanisms for doing so include public insurance, social insurance, and community-based health insurance.3 A government could choose to invest in health financing by creating a new insurance scheme, expanding coverage of existing insurance to new patient populations, or by expanding the range of services covered under existing schemes.
Resource management entails overseeing the inputs that go into the provision of health care, such as human resources and labor, pharmaceuticals, and medical technologies.14 The government can invest in the management of resources by purchasing these resources (e.g. through the procurement of drugs or hiring of doctors), or by improving systems that oversee resources (e.g. budgeting tools, health information systems) or that deliver them (e.g. through supply chain management systems).15
Healthcare and public health services refers to all of the activities actually involved in delivering care to patients and which can be facilitated by strengthening health systems. These activities include doctor’s visits, surgeries, health education and training for citizens, and the distribution of relevant health-related products. Governments also invest in specific services that generate value for money and value for many – for example highly cost effective interventions that have population impact. These include health promotion to change risk behavior (for example to stop tobacco smoking, reduce alcohol intake, exercise, eat healthy food, undertake physical activity, practice safe sex, among others), prevention services (immunization, voluntary male circumcision, condom use, use of insecticide treated nets, for example), and treatment (such as antiretroviral treatment for HIV, treatment for tuberculosis, malaria, chronic illness – high blood pressure, heart disease or diabetes mellitus for example) and care.
Several investment frameworks have been developed to identify “good buys”, for example those identified by the Lancet Commission on Investing in Health16; UNAIDS HIV Investment Framework17; STOP TB Strategy18; the Global Strategy for Women’s and Children’s Health spearheaded by the UN Secretary General19; interventions identified in the Global Malaria Action Plan20; and the Package of Essential Noncommunicable Disease Interventions (also known as WHO-PEN).21
How Should the Government Allocate Its Financial Resources for Health?
Of course, when deciding where to allocate resources for health, policymakers face many questions. Some relate directly back to the question of equity. For example, one must consider whether policy interventions should target populations that are poor or middle-class, urban or rural, working-age or the young and elderly? Others relate to the effectiveness and efficiency of the system. Should the government prioritize investment in health systems, in expensive interventions which lead to guaranteed improvements in outcomes, or in less expensive intervention that have some risk of failing? With regards to responsiveness, policymakers might face a dilemma when they decide whether to implement an effective intervention that may conflict with local cultural norms and demands.
Unfortunately, there is no algorithmic formula for determining which health interventions or areas to prioritize, and limiting analyses to comparisons of cost-effectiveness is insufficient. Without universal consensus on principles for prioritization, governments need another approach to make allocations and justify their decisions.22 Accordingly, several ethicists have proposed a framework known as “accountability for reasonableness” (A4R) to guide this decision-making process. A4R is a process, grounded in democratic principles, which aims to legitimize decision-making among “ ‘fair-minded’ people who seek mutually justifiable terms of cooperation.”23
A4R has four key conditions, which we quote from Gruskin and Daniels (2008) below:
Publicity condition: Decisions that establish priorities in meeting health needs and their rationales must be publicly accessible.
Relevance condition: The rationales for priority-setting decisions should aim to provide a reasonable explanation of why the priorities selected were determined to be the best approach. Specifically, a rationale is reasonable if it appeals to evidence, reasons, and principles accepted as relevant by fair-minded people. Closely linked to this condition is the inclusion of a broad range of stakeholders in decision-making.
Revision and appeals condition: There must be mechanisms for challenge and dispute and, more broadly, opportunities for revision and improvement of policies in light of new evidence or arguments.
Regulative condition: There must be public regulation of the process to ensure that conditions 1, 2, and 3 are met.
One should note that A4R does not lay out priorities for government investments, but, rather, a process for publicly and legitimately determining these priorities in order to guide investment decisions. The principles of A4R have shaped priority setting for health in many places such as: UK, where the National Institute for Health and Clinical Excellence (NICE) takes social value judgments into account when making recommendations about coverage for new treatments; Mexico, where decisions about which diseases the public catastrophic insurance should cover involve working groups that evaluate the clinical, economic, ethical, and social considerations; and Oregon where, in 2008, a Health Fund Board made a plan to insure all legal residents of the state involving a wide group of stakeholders and extremely transparent decision-making / information-sharing.
The Impact of Government Health Spending (GHS) on Health Outcomes
In the preceding sections, we have discussed the various frameworks policymakers can use to determine where to allocate resources, as well as a process for doing so. It is also instructive to examine the evidence for the potential implications of these investments. In this section, we discuss the implications of allocating resources for health on the health outcomes of the population. In the next sections, we discuss the implications of allocating resources for health on the economy and political landscape of a country.
Changes in government health spending (GHS) can have a direct impact on cause-specific mortality. For example, in low-income countries (LIC) a 1% decrease in GHS is associated with an increase of 18 deaths for every 100,000 live births in the neonatal period and 98 deaths before the age of five for every 100,000 live births.24 The statistical significance of this result held even when controlling for economic conditions, infrastructure, infectious disease rates, and private health spending rates. Similar results were found when only examining infant mortality in Africa and, with slightly less extreme results, for high-income countries (HIC).25 Globally, a 1% increase in GHS is also associated with a significant decrease in cerebrovascular deaths.24,26 And research among European Union countries has found that a 1% decrease in GHS is associated with increased maternal mortality.
Research coming out of IMF also suggests that increasing GHS and improving its efficiency can increase overall life expectancy in a country.9 For example, among African nations below the regional average for GHS, increasing GHS to the regional average would improve health adjusted life expectancy (HALE) by 1.2 years. In Asia / Pacific, this figure would improve by 0.9 years, and in Middle East / Central Asia, this figure would improve by 4.1 years. In addition, among African nations below the regional average for efficiency in GHS, increasing efficiency to the national average would result in an increase in HALE by 1.5 years. In Asia / Pacific, this figure is 1 year, and in Middle East / Central Asia, this figure is 1.3 years.
Achieving the health systems goal of financial risk protection through universal health coverage (UHC) can also improve population health status. Cross-country statistical evaluation of the influence of insurance coverage on health outcomes suggests that financial coverage has a causal influence on health, especially for low-income individuals, who gain better access to necessary care when they receive coverage.27 Examination of individual countries’ experiences implementing UHC supports this finding. For example, Thailand’s Universal Coverage Scheme (UCS) included benefits such as inpatient and outpatient care, surgery, accident and emergency visits, dental care, diagnostics, prevention and health promotion, and medications, and UCS increased utilization of many health services, including inpatient and outpatient visits.28,29 UHC in Turkey improved access to maternal and child health services, resulting in a significant decrease in infant mortality, as well as an improved ratio of physicians-to-patients across the country.12
Similarly, across many Latin American countries, health has been established as a constitutional or legal right, and many countries have expanded primary care as part of a platform universal health coverage.30 This push for universal coverage has led to significant decreases in infant mortality, under-5 mortality, and maternal mortality across most Latin American countries between 1990 and 2010.
Finally, one should note that efficiency and effectiveness in treating specific sets of disease can change over time as medical technologies and approaches to care delivery shift.31 For example, treatments for cataracts and depression have shown increases in the productivity of care following a decrease in per-case treatment costs. In contrast, per-case treatment costs have increased for other complex treatments and procedures, such as those associated with childbirth, but the improved health outcomes associated with these costs make the investments worthwhile.
These data provide empirical evidence that governments can directly promote improved health outcomes for citizens through government health spending, but policymakers must allocate funds wisely in order to achieve their desired outcomes.
The Impact of Improved Health on the Economy
Evidence also suggests that improved population health has positive economic impacts for a country. Since, as we have already shown, GHS can have a positive impact on population health, one might argue that GHS has a “return on investment” in the form of stronger economic output for the country. Evidence for the linkage between health and increased economic output exists at both the microeconomic and macroeconomic level.
At the microeconomic level, better health can improve the financial prospects for individuals and households.6 In particular, malnutrition, frequent illness, and unstimulating home environments can limit the physical and cognitive development of a child. On the other hand, proper nutrition and health allows for the adequate physical development of children and improved performance in school. Thus, investments at an early age “help to raise the potential for long-term academic and workplace success and lifelong well-being.”6 Among working individuals, research using the cost-of-illness approach indicates that falling ill can have direct, negative consequences for their income. The mechanisms linking ill health to reduced income include decreased productivity at work, long-term separation from the work force, and disengagement from other economic activities. Interventions targeting specific diseases and conditions, such as deworming for school children, iron supplements and iodine to treat malnutrition, and malaria prevention can all lead to improved education or income outcomes for individuals.7
Macroeconomic evidence also supports the idea that investing in health generates positive economic returns.7 In particular, there are four channels through which investments in health might improve the overall economic state of a country, all of which are corroborated by the microeconomic evidence described above. First, ceteris paribus, a healthy workforce will have higher labor productivity than an unhealthy workforce due to increased energy and reduced illness-related absenteeism. Second, a healthy population has increased educational opportunities, and education levels have a direct impact on income growth for a country. Third, populations with high life expectancies will tend to save more for the future and likely will have more working years. These increased savings can lead to increased investable capital, an important driver of growth.
Fourth, health investments that change mortality rates and total fertility can lead to demographic shifts which benefit the economy through a mechanism known as the “demographic dividend.” Often, when a country experiences a sudden improvement in health (e.g. due to the introduction of a new set of vaccines), the total fertility rate remains high for a while, but the infant mortality rate declines rapidly. This dynamic leads to a “baby boom.” Eventually, fertility rates begin to decline as couples realize that more of their infants will survive, and the original baby boom cohort reaches working age. Thus, the ratio of working-age to non-working-age people in the country increases and productive capacity increases on a per capita basis. In other words, countries that experience this demographic shift have a greater percentage of the population contributing to the economic output at any given time. Assuming that the country has or can create certain conditions to enable productivity of this working-age group (e.g. proper educational opportunities), the country will experience a “demographic dividend” that leads to its growth. This demographic dividend accounts for up to one-third of the economic boom that many East Asian countries experienced between 1965 and 1990.
Expenditures on antiretroviral therapy (ARVs) for people living with HIV/AIDS provide a useful case study of a health investment with significant health and economic returns.32 By the end of 2011, 3.5 million patients were on ARVs co-financed by the Global Fund, and 80% of those patients lived in 20 African countries. The total cost of treating these patients from 2011 to 2020 is estimated at $14.2 billion. This health investment will save up to 18.5 million life-years. Further, it will yield up to $34 billion in economic benefits (for a net benefit of up to $19.8 billion) through three primary channels: $31.8 billion in labor productivity improvements, $0.83 billion in orphan care costs averted, and $1.4 billion from the delay of end-of-life care.32
The Impact of Health Investments on the Political Landscape
Without question, the process of formulating health policy and allocating resources to health depends on the political structure and climate of a country, and, as such, has implications for the country’s political outcomes. Although a complete analysis of the way that politics and health systems reform shape each other is beyond the scope our analysis is here, it is instructive to point out explicitly that the two do matter for each other.5 Political processes shape health sector reform, and health sector reform (or lack thereof) has direct and indirect consequences for politics and politicians. For example, the move towards universal health coverage (UHC) has had distinct positive political benefits in many countries over the last several decades.33 (Figure 2 provides an overview of programs implementing UHC and the reasons for doing so in various countries.) In this section, we consider three case studies where health policy had direct implications for the political process: Turkey, the UK, and Brazil.
Box 1: Turkey’s Health Transformation Program
In the 1990s, Turkey faced three distinct but related problems related to its health system: inadequate and inequitable financing of the system, an absolute shortage and inequitable distribution of physical infrastructure and human resources, and disparities in health outcomes, especially between the east and west.12 For example, under-5 mortality rates in 1998 were 75.9 deaths per 1000 live births in the less-developed east and 38.3 deaths per 1000 live births in the more developed west. In addition, a major earthquake in 1999 left 17,000 dead and another 500,000 homeless, thereby exposing major faults in the government’s ability to manage and deliver services.
Turkey’s 2002 elections resulted in a majority for the Justice and Development Party, ending a decade of ineffective coalition governments. In 2003, as part of a broader objective to improve the economy and the government’s functioning, the Ministry of Health (MoH) introduced a Health Transformation Program (HTP) to help achieve UHC. Motivation to enact these changes, including improvements in the health system, came directly from public pressure, and failing to achieve these goals would have resulted in significant public backlash.34 Further, the public expressed high levels of dissatisfaction with the health system, with only 39.5% of people indicating they were satisfied with quality of care in 2003. Accordingly, the government displayed high levels of political commitment to this effort, with the Minister of Health visiting 81 provinces at the beginning of the HTP to meet with local government and agree to HTP implementation plans.
The HTP aimed to address challenges in a number of areas, including organization, financing, service delivery, human resources, and pharmaceuticals. The government undertook implementation of HTP using a flexible approach, focusing first on incremental and tactical changes with high visibility to citizens and later on long-term, strategic shifts that required structural changes to the system. Implementers also continuously monitored the progress of the HTP; they placed a high emphasis on citizen satisfaction with the transition, conducting focus groups, stakeholder analyses, and annual household surveys. The HTP ultimately led to significantly improved access to and usage of health services, resulting in improved health outcomes on a number of important measures such as infant and maternal mortality. User satisfaction with quality of care also increased to 79.5% by 2011. Ultimately, the successful rollout of HTP served as a blueprint for the expansion of other social services by the Turkish government, and public satisfaction with the process contributed to the government’s re-election in subsequent years.
Brazil’s Health System Restructuring During Political Transition
In the decades leading up to the re-democratization of Brazil between 1985 and 1988, the military dictatorship had generally deprioritized the protection of social rights, including health, education, and adequate living conditions.35,36 In particular, the fragmented health system left large portions of the population without access to care. Against a backdrop of general discontent with the government, a funding crisis in the social security system motivated a “public health movement” that prioritized UHC and decentralization of health delivery. Health reforms to address the system’s issues began in the 1980s. They gained a strong legal basis when the 1988 constitution formally defined health as a “citizen’s right and obligation of the state” and established the Unified Health System (SUS), which sought to unify the fragmented care delivery network into a national health system under the purview of the MoH.35
In order to appease the private sector, who opposed the government overtaking all healthcare delivery activities and who already provided care for many who had social insurance, the government focused its strategy on primary care delivery. The main component of the primary care delivery system Family Health Strategy (FHS), which consists of “multidisciplinary teams of health professionals… responsible for a defined territory and population with whom they establish contact and share responsibility for health care.”35 FHS involved transfers of funding to the municipality level based on the total number of people each municipality served (which incentivized expansion of the program to cover more people), clear roles and responsibilities at different levels of government, and a robust monitoring and evaluation (M&E) system that supported continuous improvement. The government made results from this M&E system publicly available in order to promote transparency and accountability to the public. This strategy has served expanded deliver healthcare to the poor and to place an emphasis on preventative care, although many are still left behind. Today, 75% of Brazil’s population, or 195 million people, receive services and coverage from SUS.37
Today, Brazil is facing high levels of dissatisfaction once again. In the past two years, the public has staged protests against low GHS and a system which, once again, has become fragmented and somewhat unresponsive.37 In the 2014 general election, the incumbent President, Dilma Rousseff, was re-elected by a narrow margin despite this public dissatisfaction of government resources, and many attribute her successful re-election to her government’s focus on anti-poverty programs.38 She now has the challenge of fulfilling campaign promises to use increased government revenues to raise healthcare spending, with a particular focus on improving the quality and number of public hospitals and healthcare professionals.
Public Engagement with UK’s NHS
The UK’s National Health Service (NHS) provides an example of a health population deeply engaged in the political dimensions of health delivery.1 A proud establishment of the UK’s public sector, the NHS is generally ranked as a high-performing health system among high-income countries.39 Further, an overwhelming majority of the population supports the existence of the NHS and its founding principles, with 89% of the public agreeing with the idea of a tax-funded national health system which the government runs. In spite of this broad support, however, the NHS still faces a number of challenges with regards to user satisfaction and future directions. On the one hand, 65% of the population is satisfied with the care they receive, and only 28% of the public reports worsening standards of care among the NHS. At the same time, however, 51% of the public believes that the NHS “often wastes money,” and this figure exceeds 60% for individuals over age 48. Accordingly, 58% of the public would not support spending cuts to other public services in order to increase spending for the NHS. These perceptions vary by the level of engagement with NHS, with individuals who have received more care from the NHS having better views of the organization than those who have had less contact with the system.39
The high level of engagement among the public with the NHS, coupled with some perception issues, poses a challenge to the NHS, particularly as it faces a funding issues. Indeed, projections show that by 2030, the NHS will have a £65 billion funding gap. In addition, the NHS will face four key transitions that will force the government to rethink the structure and role of the NHS: a demographic transition to an older population, an epidemiologic transition to more chronic illness and multimorbidity, an economic transition with a widening income gap across the country, and a social transition to a public that places a high degree of value on responsiveness of the system and personalization of care. UK policymakers will have to balance the competing health, financial, and social demands placed on the NHS in order to maintain its relevance going forward.39
Figures
Figure 1. Health systems functions, outputs, and outcomes.
Figure 2. Representative list of reforms implementing universal health coverage.
Country
Year
UHC Reform
Political timing / reason
High-income countries
UK
1948
Tax financed National Health Service with universal entitlement to services
Welfare state reforms of new government following Second World War
Japan
1961
Nationwide universal coverage reforms
Provide popular social benefits to the population
South Korea
1977
National health insurance launched
Flagship social policy of President Park Jung Hee
USA
2012
National health reforms designed to reduce number of people without health insurance
Major domestic social policy of the President
Low- and middle-income countries
Brazil
1988
Universal (tax-financed) health services
Quick-win social policy of new democratic government
South Africa
1994
Launch of free (tax-financed) services for pregnant women and children under six
Major social policy of incoming African National Congress Government
Thailand
2001
Universal coverage scheme extends coverage to the entire informal sector
Main plank of the populist platform of incoming government
Zambia
2006
Free health care for people in rural areas (extended to urban areas in 2009)
Presidential initiative in the run up to elections
Burundi
2006
Free health care for pregnant women and children
Presidential initiative in response to civil society pressure
Nepal
2008
Universal free health care up to district hospital level
Flagship social policy of incoming government
Ghana
2008
National Health Insurance coverage extended to all pregnant women
Leading up to a Presidential election
China
2009
Huge increase in public spending to increase service coverage and financial protection
Response to growing political unrest over inadequate coverage
Sierra Leone
2010
Free health care for pregnant women and children
Presidential initiative which was a major factor in recent elections
Georgia
2012
Extending health coverage to all citizens
Key component of new Government’s manifesto
References
Atun, R., The National Health Service: value for money, value for many. Lancet, 2015. 385(9972): p. 917-8.
Etienne, C., A. Asamoa-Baah, and D.B. Evans, Health systems financing: The path to universal coverage. 2010: World Health Organization.
Gottret, P.E. and G. Schieber, Health financing revisited: a practitioner’s guide. 2006: World Bank Publications.
The World Bank. Indicators. 2015 [cited 2015 March 23]; Available from: http://data.worldbank.org/indicator.
Roberts, M., et al., Getting health reform right: a guide to improving performance and equity. 2008: Oxford university press.
Jack, W. and M. Lewis, Health investments and economic growth: Macroeconomic evidence and microeconomic foundations. World Bank Policy Research Working Paper Series, Vol, 2009.
Bloom, D. and G. Fink, The economic case for devoting public resources to health. Manson’s Tropical Diseases, 2013: p. 23-30.
Atun, R. and S. Fitzpatrick, Advancing Economic Growth: Investing In Health. A summary, 2005.
Grigoli, F. and J. Kapsoli, Waste not, want not: the efficiency of health expenditure in emerging and developing economies. 2013.
Cutler, D.M., A.B. Rosen, and S. Vijan, The value of medical spending in the United States, 1960–2000. New England Journal of Medicine, 2006. 355(9): p. 920-927.
Abiola, S.E., et al., Survey in Sub-Saharan Africa shows substantial support for government efforts to improve health services. Health affairs, 2011. 30(8): p. 1478-1487.
Atun, R., et al., Universal health coverage in Turkey: enhancement of equity. The Lancet, 2013. 382(9886): p. 65-99.
World Health Organization, The World health report: 2000: Health systems: improving performance. 2000.
Hsiao, W.C., Abnormal economics in the health sector. Health policy, 1995. 32(1): p. 125-139.
Shakarishvili, G., et al., Health systems strengthening: a common classification and framework for investment analysis. Health Policy and Planning, 2011. 26(4): p. 316-326.
Jamison, D.T., et al., Global health 2035: a world converging within a generation. The Lancet, 2013. 382(9908): p. 1898-1955.
Schwartländer, B., et al., Towards an improved investment approach for an effective response to HIV/AIDS. The Lancet, 2011. 377(9782): p. 2031-2041.
Raviglione, M.C. and M.W. Uplekar, WHO’s new Stop TB Strategy. The Lancet, 2006. 367(9514): p. 952-955.
Ki-Moon, B., Global strategy for women’s and children’s health. New York: United Nations, 2010.
Roll Back Malaria, The global malaria action plan. Roll Back Malaria partnership, 2008.
World Health Organization, Package of essential noncommunicable (PEN) disease interventions for primary health care in low-resource settings. 2010.
Daniels, N., Accountability for reasonableness: Establishing a fair process for priority setting is easier than agreeing on principles. BMJ: British Medical Journal, 2000. 321(7272): p. 1300.
Gruskin, S. and N. Daniels, Process is the point: justice and human rights: priority setting and fair deliberative process. American Journal of Public Health, 2008. 98(9): p. 1573.
Maruthappu, M., et al., Government Health Care Spending and Child Mortality. Pediatrics, 2015: p. peds. 2014-1600.
Anyanwu, J.C. and A.E. Erhijakpor, Health Expenditures and Health Outcomes in Africa*. African Development Review, 2009. 21(2): p. 400-433.
Maruthappu, M., et al., Unemployment, government healthcare spending, and cerebrovascular mortality, worldwide 1981–2009: an ecological study. International Journal of Stroke, 2015.
Moreno-Serra, R. and P.C. Smith, Does progress towards universal health coverage improve population health? The Lancet, 2012. 380(9845): p. 917-923.
Hanvoravongchai, P., Health financing reform in Thailand: toward universal coverage under fiscal constraints. 2013.
Limwattananon, S., et al., Why has the Universal Coverage Scheme in Thailand achieved a pro-poor public subsidy for health care? BMC Public Health, 2012. 12(Suppl 1): p. S6.
Atun, R., et al., Health-system reform and universal health coverage in Latin America. The Lancet, 2014.
Cutler, D.M. and M. McClellan, Productivity change in health care. American Economic Review, 2001: p. 281-286.
Resch, S., et al., Economic returns to investment in AIDS treatment in low and middle income countries. PloS one, 2011. 6(10): p. e25310.
Yates, R. and G. Humphreys, Arguing for universal health coverage.
Atun, R. and S. Sparkes, Fixing a Broken Health System: Confronting Health System Challenges in Turkey. Harvard School of Public Health: Executive and Continuing Professional Education: Boston, MA.
Couttolenc, B. and T. Dmytraczenko, Brazil’s primary care strategy. 2013.
Paim, J., et al., The Brazilian health system: history, advances, and challenges. The Lancet, 2011. 377(9779): p. 1778-1797.
Kepp, M., Upcoming election could rekindle health debate in Brazil. The Lancet, 2014. 384(9944): p. 651-652.
Gomez, E.J. Why Dilma Rousseff was re-elected in Brazil. 2014 [cited 2015 April 1]; Available from: http://www.cnn.com/2014/10/27/opinion/gomez-rousseff-election-win/.
Gershlick, B., A. Charlesworth, and E. Taylor, Public attitudes to the NHS: an analysis of responses to questions in the British Social Attitudes Survey. 2015, The Health Foundation: London.
Gabriel Seidman, Doctor of Public Health candidate and Centennial Fellow
Governments worldwide are under public pressure to provide universal access to affordable, reasonable quality health care. This poses challenges for most governments including the role of the state in health care delivery, levels of coverage for people who cannot afford to pay out of pocket, and most particularly the ability of the state to subsidize health care costs. As a result, many governments turn to private sector health insurance and service providers to complement public health care provision.
Private sector financing and delivery of health care exist in all nations. Private sector financing includes patients’ out-of-pocket payments, private insurance, and free or reduced cost health care delivered by charity hospitals/clinics. On the health care delivery side, private hospitals, clinics, pharmacies and indigenous practitioners could be major suppliers of health care.
The private sector could strengthen the delivery of public health services, but it could also be a hindrance. That depends on whether the government knows how to harness the strong points of the private sector to serve the well-being of society. The private sector may possess the capital and the desire to invest in health facilities, as well as superior knowledge and management skills to manage insurance operations, functions of hospitals and clinics, and construction of facilities. The private sector could also be relatively free of corruption in its operations. On the other hand, the private sector could damage the publically financed health services delivered by private providers charging exorbitant prices, garnering excess profits by exploiting patients’ ignorance of medical needs, and siphoning off the most skilled physicians and nurses from the public sector with much higher compensation.
“Private sector” is a broad term. By their nature, private sector organizations, including for-profit, charity (non-profit) and hybrid entities, behave very different than public sector organizations. We should clearly recognize that for-profit organizations have the obligation to produce the highest profit for their investors (e.g. stockholders.) and they may use any legal means to generate the largest profit. The organizational goals of charity organizations are different; they are not pursuing profits but instead, they aim to financially break-even while serving noble social purposes. Hybrid organizations could be pursuing profits as well, but a portion of the profit is allocated for charity, such as providing free health services for the poor. Well-known examples of these organizations are the Aravind Eye Hospital and the Narayana Heart Hospital in India.
This note serves two purposes. First, it gives a concise explanation of the roles of the private sector in public health care by organizing private sector activities into different types. We examine the evidence of the contributions, if any, that the private sector has made for public interest. Second, we present vexing health policy problems confronted by three nations and asking whether these nations can be better off by leveraging the private sector to deliver public health services. If so, how should they do it?
Types of public service delivery by the private sector
Historically, most nations have had a mixture of public and private financing and provision of health care. In developing nations, we have a large number of faith based charity hospitals and clinics. However, the public and private sectors had traditionally been very much separated. The government financed, directly managed and delivered health services in public facilities, while private providers charged patients directly for services delivered in private facilities. Often, the publicly financed and directly managed public facilities were inefficient and not responsive to patients’ preferences because they were public monopolies and managed with rigid bureaucratic rules. In the worst cases, political interference, patronage and corruption crept in.
The following are the major types of how private sector engaged in public health services:
1) Purchaser/Contractor model for public health services
A new idea of how to reform publically financed and directly managed public health facilities swept the world 25 years ago: separate financing from delivery of services. The government would finance health care for equity reasons or/and for pooling risks, but would purchase/contract from public and private providers for the provision of services. This required autonomous governance of public facilities so that public facilities can compete with private facilities on costs and quality of health care. In this model, the government reduces its bureaucratic management of public hospitals and replaces it with management by independent boards with community representatives. A good example is England’s Foundation Trust model. The purchaser (e.g. England’s NHS) represents the public interest and negotiates with the public and private providers for the lowest prices and the best outcomes performance.
This new conceptual approach brings up an array of complex issues such as: 1) Who can be the most effective purchaser for the public interest? 2) What information and negotiation skills must the purchaser possess? 3) How much is the administrative cost for purchasing/contracting versus directly managing public facilities? 4) How can quality of health care and health outcomes be defined, and what quality and health outcomes can be measured for a contractual agreement?
Current evidence about the benefits of the purchaser/contractor model varies from very positive to negative, depending on the types of services to be contracted and the ability of the government to negotiate and contract as compared to its capability to manage and deliver public health services. The most positive results of the purchaser/contractor model were found in war torn nations after World War II where public health services may have largely been destroyed. In those situations, the government uses donor funds to purchase vaccination and maternal and child health services from private sector providers. There are also several cases of success when purchasers use pay-for-performance payment methods for delivery of primary care services or for delivery of selected medical services such as imaging tests and hip or knee replacements. On the other hand, there have been numerous cases where the purchasers paid excessive prices and received low quality services from the private providers.
2) Concession model
Concession is a relatively new approach to leverage the private sector for public service delivery. When a government has difficulties providing adequate capital investments for public health facilities, it may give a long-term concession to a private for-profit firm to jointly fund public facilities and for the private firm to manage the facilities. The firm will receive a guaranteed annual payment for delivering a specified minimum volume of specified quality of health services. If the private firm can improve the productive efficiency and reduce costs, the firm can earn a handsome profit. Meanwhile, the government would not pay more than what it originally budgeted for. The concession model can have various degrees of concession. The best-known case is the Lesotho case which is described in greater detail below. Brazil and Egypt have also tried the hospital concession model. However, the concession model is a recently developed approach, we do not have solid and objective evidence about its performance.
Lesotho Case
By year 2000, it became apparent that Lesotho’s national referral hospital in the capital, Queen Elizabeth II Hospital (QEII), had to be replaced. According to Timothy Thahane, the Minister of Finance of Lesotho at that time, the deteriorating infrastructure and high hospital operating costs forced a large number of patients to be transferred to nearby South Africa for treatment. At the same time, doctors were also leaving for South Africa because of the poor working conditions and low compensation. The Lesotho government had to address these serious problems. However, the government lacked adequate funds to rebuild the capital’s hospital and to increase physicians’ compensations. Minister Thahane made a case for leveraging private sector investment and management know-how to rebuild and renew QEII. He had to overcome the strong reservations of governmental health leaders and health professionals who had looked at health care as a government responsibility with little role for the private sector.
After a long deliberation, the Lesotho Government issued a tender for private sector investment, posing the following question to the private sector: for the level of expenditure at QEII at that time, how much would the private sector be willing to invest in a hospital, and how much more could the private sector provide in volume, quality, and range of medical services? Several private companies rose to this challenge and bid on the project.
Lesotho lacked lawyers, financial experts as well as negotiation experts to negotiate and prepare contracts. Consequently, Lesotho relied on the analysis and advice from the consultants provided by the International Finance Corporation, the private financing arm of the World Bank, in the negotiating and contracting.
Tsepong (Pty) Ltd, a consortium comprised of the private South African hospital operator Netcare and local partners won the bidding. The resulting contract, signed in 2008, was a concessional package with a joint private and public investments and private management of a new hospital. Tsepong would finance 62.3% ($95.4 million) of the new capital investment needed, with the Lesotho government providing the remaining 37.7% ($57.7 million), for a total investment of $153.07 million. Tsepong would be responsible to design, build and construct a 425-bed (390 public beds, 35 private beds) hospital, the Queen ‘Mamohato Memorial Hospital (QMMH) to replace QEII. Tsepong would also responsible for the renovation, re-equipping, and operation of three primary healthcare filter clinics in the capital area. Private and public beds would differ only in their amenities (e.g., privacy, television).
Under the contract, Tsepong would manage and provide all clinical and non-clinical services for QMMH for 18 years. The government would pay Tsepong an annual fixed service payment of $30.3 million towards capital repayment, operating expenses and for delivery of all services, indexed to increase with inflation rate. The unitary payment decided upon was based on the number of outpatients and inpatients treated. The contract would require approval for any patients that exceeded the aforementioned agreed number of patients. According to government officials who were involved in the negotiation, this initial annual payment is approximately equal to what the government expected to pay for services of QEII. After eighteen years, QMMH will be turned over to the government. Maintenance and replacement schedules were also established in the PPIP contract such that equipment and technology will still be current at the end of the 18-year contract in 2026.
Tsepong agreed to treat all patients who present at the hospital and 3 filter clinics, up to a maximum of 20,000 inpatients and 310,000 outpatients annually. The private operator is responsible for the delivery of all clinical services with only a few exceptions. Tsepong has full authority over human resources, including the recruitment and retention of doctors, nurses, and other health professionals; it also responsible for all medical equipment, pharmaceuticals and supplies. Under the contract, patients can be seen at QMMH only by referral, either from the three filter gateway clinics, or from other district hospitals or private practitioners. The QMMH referral system was developed to support a primary care based health care system that directs patients to the primary care clinics and they refer complicated and serious patients upward. Such a system would be most cost-effective and also manage the demand for hospital services.
Under the terms of the contract, QMMH and the 3 filter clinics would collect the Ministry of Health set user fees from patients. Tsepong would remit these fees to the national Treasury just as public district hospitals and health centers do. User fees at QMMH remain the same as at any other public facility in the country, thus achieving cost neutrality for the patients.
The project has an independent monitor, a unique role specifically jointly created and appointed for this project by the government and Tsepong. This monitor performs a quarterly audit of Tsepong’s performance against the contractual performance indicators and determines penalties where performance has not been achieved.
Interim Result: The new hospital, QMMH, was constructed successfully and started its operation with some delay in October, 2011. However, there is a controversy about whether QMMH is achieving its original goals. The hospital reached its maximum capacity very early when its tertiary services attracted patients to flock to the hospital without proper referrals, regardless of whether they needed the expensive and sophisticated tertiary services provided by QMMH. Resources were thought to be wasted while other patients who needed QMMH services were not able to access them. To mitigate that situation, the Lesotho government realized that it had to reform its whole health care system for QMMH to function properly as a tertiary hospital. As a result, while QMMH were opening its doors in 2011, the Lesotho government also undertook a major investment and effort to renovate and improve more than 150 health facilities, including 138 primary health centers.
3) Outsourcing models
Managing and operating a social health insurance program require capable managers and many experts, including physicians, actuaries, insurance risk analysts, information technologists, claim operation managers, accountants, etc. International experience shows that may take a decade for a new social insurance program to establish sound operating systems and a capable administrative organization.
Managing and operating a large hospital faces a similar challenge. Hospital management consists of a set of complex functions. It requires a team of leaders who understand clinical medicine and how to organize, motive, and manage the back-bone of any hospital– the numerous physicians who are autonomous professionals. At the same time, the hospital has to satisfy patients’ expectations and demands, assure quality of services, maintain its financial soundness, plan its future, etc. Operationally, hospitals are not just providing medical services, they have to run hotel services for hundreds if not thousands of patients, food, laundry, internal security, IT services, etc. Hygiene and sanitation are also of paramount importance.
When does the government possess the know-how and the capable human resources to manage and operate social insurance programs or public hospitals efficiently and effectively? If a government does not have the capability, would it better for the government to outsourcing the function to the private sector? In some cases such as food service and cleaning, private companies specialize in these particular function might enjoy the economies of scale and can produce the service cheaper.
For efficiency and effective gains, many nations outsourcing several key functions to the private sector. We give illustrations of three types of outsourcing:
A. Outsourcing administration of social health insurance
Fifty years ago, the USA established the social health insurance for the elderly (i.e. the US Medicare program). The government decided to outsource the administration of the health insurance to private health insurance firms because the government lacked the knowledge, technical expertise, and skills to manage such a large and complex insurance operation that involved more than 400 million of medical interactions between patients and physicians/hospitals each year. The United States also decided to outsourcing for political reasons; it reduced the opposition of the health insurance industry against the passage of the Medicare program.
For developing nations where the government’s capacity is weak, particularly if patronage and corruption is widespread, the government will not be able to administer any social health program efficiently and effectively. The nation has to consider leveraging the private sector to implement and administer the country’s social health insurance program. Recently, when India introduced its social health insurance for the poor, it also outsourced the insurance administration to private firms.
However, nations that have capable and effective governments found the costs of public administration of universal health insurance are less than the private sector. It incurs less administrative costs. Good cases include Canada, Taiwan and China.
B. Outsourcing specific departmental functions
The government can outsource certain functions to private firms and improve the efficiency and quality of public health services. Sometimes private firms can specialize in the production of certain products or services at a lesser cost. For more than thirty years, public and private hospitals in advanced economies found that outsourcing cleaning, laundry, internal security, and food services to private firms that specialize in these services can reduce their costs. More recently, small hospitals and clinics found that outsourcing laboratory services to private clinical laboratories can reduce their costs.
C. Outsourcing management of public facilities
Outsourcing hospital management is a more recent type of outsourcing to gain greater efficiency is management. A good example is Battagram, a poor district in Pakistan, which wanted to improve its primary healthcare services through better management of the public facilities and health workers. The Department of Health of Battagram contracted out management/delivery of primary healthcare services to a NGO–Save the Children USA. Battagram used donor funds to contract the NGO who agreed to provide a package of primary care services. The NGO was given the full administrative control of the staff and operations of the district health facilities, responsible for paying the staff and procurement of medicines, supplies and equipment. It’s one of the few contracting arrangements where salaries of government staff were paid through the NGO.
With the flexibility to use funds across budget lines, Save the Children paid staff a salary based on the market rate—roughly triple the government rate—plus a bonus for good performance. The NGO was able to increase the number of medical staff by 53%, especially recruiting female health staff and strengthening community-based outreach to address gender constraints in a traditional society. As a result, people gained much greater access to primary care. Pakistan plans to replicate this outsourcing of management to other districts.
Kenya
Kenya, a nation of 41 million people, has made significant improvements in prevention and primary care that resulted in impressive reductions in infant mortality and controlling HIV/AIDS. Kenya has also been planning a national health insurance (NHI) program to achieve Universal Health Coverage (UHC) by 2030. In this effort, it has chosen to prioritize the coverage of poor people and maternal health care first. Meanwhile, the new Kenyan Constitution has decentralized the budget, power, and responsibilities from the national government to forty-seven counties. As a result, the management and operation of public health services (staff and facilities) is being devolved to the counties. The NHI plans to purchase and contract public and private providers for services. The key question is: should Kenya rely on the existing government social health insurance agency—the National Hospital Insurance Fund (NHIF) — to administer the National Health Insurance?
The NHIF was established in 1966, aiming to eventually offer a social health insurance to all Kenyans. However, NHIF suffered a long history of mismanagement with patronage and corruption. NHIF spent more than one-half of its annual premium revenue for administrative expenses, while the international average is about 10% for developing nations. In the 2003 scandal when the Euro Bank collapsed, the biggest casualty was the NHIF, which lost Sh479 million of its insurance reserve fund in the collapse. Executive members of the NHIF were accused of being involved in the collapse of the bank itself. More recently, in 2011, the NHIF was supposed to use tenders to purchase and contract the most competent and efficient providers. However, the Parliament’s subsequent investigation showed that the NHIF awarded Sh318 million to two controversial private firms operating private clinics. The Central Organization of Trade Unions revealed that the NHIF money was awarded to some non-existent clinics while it was also found that 77 illegal clinics were licensed to receive money from the NHIF.
Recently, Kenya is trying to reform the NHIF agency with changes in governance, organization and management. The reform of the NHIF is moving forward, albeit slowly. The latest figures show that the NHIF still spend 40% of its premium revenue on administrative costs.
What would you do as the Kenyan Minister of Finance? Given the NHIF is the only public agency with the technical know-how to administer National Health Insurance, would you give the administration of the National Health Insurance to the NHIF or outsource the administration to a private insurance firm?
South Africa
South Africa is a middle income nation with two separate health systems. Sixteen percent of the people, mostly affluent households, pay for private health insurance to finance their health care. They obtain their health services from private clinics and hospitals. Each year, roughly one-half of South Africa’s total national health expenditure is spent on this 16% of the population. The other eighty-four percent of the population relies on publically financed and publically managed health care. There is a great disparity in health care between these two groups.
The South African government has been planning the introduction of a National Health Insurance program (NHI) since 2011 to achieve UHC, advocating healthcare as a public good that should be provided by the state. NHI’s aim is to ensure that South Africa progresses towards UHC and all its citizens have access to appropriate, efficient and quality health services.
South Africa faces poor management, inefficiency and corruption in its public health services. According to Health Minister Aaron Motsoaledi, the most corrupt health departments among the nine provinces in the country are Limpopo, Gauteng and the Eastern Cape. For example, in early 2013, newspapers reported a set of devastating corruption incidences in the Eastern Cape Health Department: 544 of the 8,034 department workers were suspected to be ghost employees, 929 department employees were listed as suppliers for the health department, 235 had received payment of R42.8 million from the department for unidentified purposes. The department said there were 35 spouses of employees doing business with the department, and linked to 35 companies which received payments of R11 million.
Similar to the provincial health departments, in some provinces, public hospitals also experience mismanagement and corruption. Public hospitals are highly stressed institutions with poor quality of health services due to inadequate funding, staff shortages, unmanageable workloads and management failures. Meanwhile, the healthcare outcomes produced by South Africa’s private healthcare sector have been such that it has been ranked alongside the healthcare sectors of countries such as Australia, Sweden, Belgium, Switzerland and Ireland.
The Ministry of Health is currently fully committed to better governance and management to root out corruption, as well as improving efficiency and quality of health care delivered by the public facilities. The Ministry of Health is also likely to be responsible for the implementation and management of South African National Health Insurance (NHI) when it passes into law.
Given the lack of experience and technical capacity in the government for administration of the NHI and the history of corruption within some provincial and district health departments, what would you do? Would you entrust the administration of the NHI and service delivery to the government or would you outsource them to private entities?
Ghana
Ghana implemented a National Health Insurance Scheme (NHIS) in 2004 to provide more equitable access and financial coverage for basic health services. People have to pay a premium to enroll into the NHIS and the premiums vary with household income; children under age 18 and elderly over age 75 are subsidized by the government and they do not have to pay. Most people are enrolled through the District Mutuelle Health Insurance Scheme (DMHIS) which operates in every district in Ghana. Each DMHIS is in charge of accepting and processing memberships, collecting premiums, and processing claims from accredited facilities. The benefit package offered by the DMHIS is comprehensive, covering up to 95 percent of disease conditions in Ghana.
The NHIS has brought many organizational and management challenges to DMHIS and hospitals. It has been reported that 72 percent of all DMHIS lacked the appropriate and adequate human resources and specialists for insurance operations, financial management, claim payment, and data management. Consequently, there has been a 3-6 month lag period between enrollment and receipt of an insurance card. Without the card, the enrollee is not eligible for benefits. As a result, many enrollees would not re-enroll. By 2010, only about 34% of the total population was an active NHIS enrollee. Providers also complained about long delays in receiving claim payments for services rendered and drugs provided. DMHIS suffered from large financial losses from low enrollment, payment of fraudulent claims for services and drugs, and high administrative expenses. The NHIS faced with deficit of more than GHC47.3 million by the end of 2011.
In 2011-12, Ghana debated a new law to reform the administration of NHIS. What would you have advised the government of Ghana to do? Would you have recommended that the administration of the NHIS be outsourced to a private entity?
*William Hsiao is the K.T. Li Professor of Economics at Harvard School of Public Health
*Maria Joachim, MSc, holds a Bachelor of Science degree in Biology from Bates College and a Master of Science in Global Health and Population from the Harvard T.H Chan School of Public Health. She is currently pursuing a PhD in Health Services Organization and Policy at the University of Michigan.
Akazili J, Gyapong J, McIntyre D. 2011. “Who pays for health care in Ghana?” International Journal for Equity in Health, 10: 26. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21708026
Birla B, Taneja U. 2008. “Public Private Partnerships for Healthcare Delivery in India.” The Internet Journal of World Health and Societal Politics, 7:1. Available at: http://ispub.com/IJWH/7/1/9363
De Costa A, Vora KS, Ryan K, Raman PS, Santacatterina M, Mavalankar D. 2014. “The State-Led Large Scale Public Private Partnership ‘Chiranjeevi Program’ to Increase Access to Institutional Delivery among Poor Women in Gujarat, India: How Has It Done? What Can We Learn?” Plos One. Available at: http://www.plosone.org/article/info%3Adoi%2F10.1371%2Fjournal.pone.0095704
Durairaj V, D’Almeida S, Kirigia J. 2010. “Obstacles in the process of establishing a sustainable National Health Insurance Scheme: insights from Ghana.” World Health Organization. Available at: http://www.who.int/health_financing/pb_e_10_01-ghana-nhis.pdf
Hor, S. 2013. “Ten years on and major pitfalls still hindering Ghana’s National Health Insurance Scheme.” Available at: http://www.globalhealthcheck.org/?p=1523
The London 2012 Olympicsi is generally regarded as the most successful Games ever. The path to success was far from smooth. One person more than any other had championed these Games for Britain for ten years, from inception to closing ceremony. Tessa Jowell, UK Secretary of State for Sport and Culture, and a senior political ally of Prime Minister Tony Blair, had overseen Britain’s successful hosting of the Commonwealth Games in 2002. With this experience, Secretary Jowell felt passionately that Britain was in a strong position to host the 2012 Olympics. She was also convinced that there could be real benefits for the country and that the Games could create a strong legacy.
The Olympics is the world’s largest sporting event on a scale far greater than any other government project. For a host city and for the government of the host country there must be gains beyond prestige. The UK government therefore planned to convert contaminated, waterlogged and derelict land in the east of London, at the heart of an effort to regenerate one of the most deprived parts of the city, into an Olympic Park with a mix of permanent and temporary venues, and accommodation for athletes and the media. London’s notoriously crowded public transport systems and roadways presented another major challenge. Overdue investment would be accelerated. Jowell was confident that with strong government support, good planning and management these challenges could be met. The far greater initial challenge was winning support across government and with the wider public.
This case explores what lay behind the success of the London Olympics. How the lessons from the Games can be applied to ministerial leadership in implementing other ambitious government priorities and projects. This case is based mainly on in-person interviews with Tessa Jowell, as well as reported interviews by other principal players in the delivery of the Games.
Building Political Support
The UK had a track record of failure in Olympic bidding. The UK put Birmingham up for the 1992 Games and Manchester for both the 1996 and 2000 Games. The bid from Birmingham and the first Manchester bid ended in embarrassment, with both coming fifth out of six competing cities. By contrast, the Manchester bid for the 2000 Games saw the city achieve a more respectable third place.ii By 2002 the International Olympic Committee (IOC) was clear that only a bid for the Games in London would be seriously considered.
The newly appointed Secretary for Sport and Culture, a seasoned politician, was impressed by the successful delivery of the Commonwealth Games and understood the “co-lateral benefits” of such major sporting events. Jowell, a progressive member of the British Labor Party, saw real potential gains for the British economy, boosting employment and regenerating a seriously deprived section of east London. She was supported in this latter objective by the Mayor of London, Ken Livingstone — known by many as “Red Ken” referring to his leftist political leaning. The Mayor saw the Games as a way of securing cash to regenerate London’s East End — an important part of his political agenda.
Prime Minister Tony Blair was a “sports nut,” but the Prime Minister was not in the early stages prepared to wage the political battle to get government and public support. Getting his support was critical. Blair told Tessa this was up to her. The Prime Minister was particularly wary of picking this battle with Chancellor of the Exchequer, Gordon Brown. Tension between the Prime Minister and Chancellor are well documented.
According to Jowell, there was little initial support in the government or the civil service for hosting the Games, and the strident criticism of the media created deep public skepticism. Jowell knew that she had to proceed strategically. She says that taking the time to persuade key players individually was essential to selling the idea. This ensured they would not feel steamrolled. If the UK was to bid for the Games the Cabinet had to own the ambition too. Over more than six months, she met individually with senior government colleagues and strategically laid out the potential benefits to each of their departmental and political priorities. Jowell’s pitch was built around the answers to four questions:
Was the project deliverable?
Was it affordable?
Would it leave a legacy?
Could we win and beat Paris?
The substance of Jowell’s pitch was that the Games would be a major shot in the arm for the UK economy with substantial additional benefits in areas such as transportation, tourism, infrastructure development and urban regeneration, as well as boosting sport, physical wellness and national spirit. The IOC would be impressed by the evidence of ambitious planned legacy. Jowell knew that it was also important to her credibility not to overplay expectations; she needed to ensure projections of the probable benefits were not mere hyperbole, but based on solid evidence. She also had to be sure that the eventual budget was sufficient and that the project could be delivered “on budget and on time.”
Jowell left the biggest challenge until the last before seeking formal Cabinet approval. The Treasury had made clear its opposition to the idea and the Chancellor avoided engagement, declining for weeks to meet with Jowell. His support was essential to persuade the rest of the Cabinet. Jowell says she deployed a combination of “persistence, charm and a flash of steel” in eventually forcing a meeting with Chancellor Brown days before the Cabinet was scheduled to consider whether or not to agree on support for the proposal to bid for the Games. The Chancellor was eventually engaged in the face of Jowell’s persistence. She at that stage knew that she already had the support of the Prime Minister and most of the Cabinet.
In May 2003 the Cabinet gave the go ahead for the bid and London became a late entry in the race to host the 2012 Olympics – with Paris still very much the lead contender. Over the next two years the bid company was established and the underpinning machinery of government was put in place to maximize success and to safeguard the necessary financial guarantees from government departments (and the opposition) to allow the London bid to proceed.
The Game is On: Marshaling Resources
Jowell, with the support of London Mayor Livingstone, set about addressing some of the most significant hurdles to a bid, namely the cost, and concerns that London had no chance of beating a better-prepared Paris. They needed more information about the likely necessary budget and jointly commissioned a consulting company, Arup, to undertake a cost-benefit analysis of a specimen Olympics. Initially, Arup reported that the Olympics would need a public subsidy of £1.1bn.iii However, by Christmas, the press was reporting that the Olympics could cost the taxpayer as much as £2.95bn. The Olympic budget caused headaches from the start. There were so many uncertainties and unanswerable questions. There could be no site surveys to assess the scale of essential remediation. The Delivery Authority which would build the Park might be liable for VAT, but that could not be settled until the technical details of its functions were clarified. At that stage, consultant advice was that project contingency would be sufficient. This was much less than the programme contingency of 60% subsequently required by the Treasury.
Jowell prepared the groundwork for public funding, agreeing with Ken Livingstone that up to £1.1bn of public subsidy would be met by London, split equally between the London Development Agency (LDA) and London council taxpayers.iv Thanks to Tony Blair’s predecessor, John Major, there was an additional source of funds potentially available which would not place a burden on the taxpayer – the National Lottery that had opened for business in 1994. Jowell also met with lottery operator, Camelot, and the Lottery Commission to discuss raising £1.4bn through an additional Olympics Lottery game. This was controversial since the decision to divert Lottery Funding of 11% from all specialist distributors plus the creation of an Olympic Lottery Fund meant less for non-Olympic programmes. This received an angry reaction from many quarters.
The task of convincing colleagues and the public that a win was possible was more difficult. Formal government decision-making about the bid process was through “Misc 12” – a cabinet committee chaired by Foreign Secretary, Jack Straw. It remained wary as the common view persisted that Paris would host the 2012 Games. Such was the concern over Paris being the pre-ordained victor of the bidding process that Jowell decided to go to Switzerland in January 2003 to seek assurances from IOC chair Jacques Rogge about whether “this [was] actually an open race or a competition that [would] lead to a Paris victory.”v He gave absolute assurance about the openness of the contest. This was important. The timing of a government decision to proceed with the bid was further complicated by the imminent military intervention in Iraq. A government decision on the Olympics was originally due in February 2003 but was delayed by three months while the potential war with Iraq obviously took main priority.
Some have argued that ironically the presumed “unwinnability” of the Games was helpful to those pressing for a London bid. After all, some reasoned when signing up, there was little risk they would have to deliver – Paris was going to win, and it was not worth antagonizing cabinet colleagues and wasting political capital opposing something that was highly unlikely to happen.
Organizing a Winning Bid
With the clock ticking down on the deadline for submission of the 2012 bids, Jowell now had to combine her role as chief political champion with that of top executive, assuming responsibility as the newly appointed Minister for the Olympics responsible for winning the bid and delivering the Games. She knew from experience that her leadership would only be as good as the team around her.
A team to lead the bid was assembled, and in line with IOC rules, a private bid company named London 2012 took charge of this. Barbara Cassani, an American businesswoman who had successfully launched British Airways’ low-cost airline, Go, was appointed by Jowell after open competition to chair London 2012. Keith Mills, described by Barbara Cassani as “one of the least known, most successful businessmen in Britain,” became Chief Executive. Between them, Cassani and Mills had just over a year to create a master plan (known as the ‘Bid Book’) that would:
Detail where events would be held and what infrastructure would be built
Provide an overall budget projection for the staging of the Games
Persuade the public to support the Games through a significant marketing campaign
They also had to organize a huge lobbying effort to convince the 115 IOC members, the electorate for the Host City 2012, that London was the right choice. Jowell recruited Sebastian Coe to lead on liaison with the IOC. Sebastian Coe, a celebrated Olympic gold medalist and a former Conservative Party member of the British parliament, was a strong addition to the team.
London 2012 was given the freedom to lead on developing the Bid Book. The company board and a monthly crosscutting committee chaired by Mills were the main interfaces with Government. It was here that London 2012 met with Government to agree on the crucial departmental guarantees that were to be signed by relevant secretaries of state, which the IOC required of all candidate cities. London 2012 was directly accountable to Tessa Jowell. Importantly, Jowell notes, there was no back channel to the Prime Minister. Jowell had been clear from the beginning that there could be no confused lines of accountability.
In May 2004, London passed the first hurdle when the IOC selected it as one of the five formal candidate cities – along with Paris, Madrid, New York, and Moscow. This triggered a change of leadership at London 2012. Barbara Cassani decided she was not suited to the next stage of the lobbying task. She suggested to Jowell that Seb Coe, as a double Olympian, would be the most powerful Bid leader. Jowell then negotiated his appointment in the face of some politically tribal skepticism. London was now moving into the final stages of the bid, finalizing details of the candidate file to be submitted in November 2004.
At this point, Coe, Mills, and other London 2012 staff stepped up their work with politicians on speeches and marketing materials that would showcase London. Politicians – most often Tony Blair, Ken Livingstone, or Tessa Jowell – were asked to give speeches according to which of them IOC members would be most impressed by. In some cases, a mayor was the most appropriate figure, while in others a prime minister or Olympics minister was a better fit. The key to these events was encouraging the individual politicians to set aside their specific objectives (e.g., the regeneration of East London) to emphasize the importance of a great and successful Games. This was by far and away the most important test for the IOC.
Even then, the UK was still perceived as the underdog. In January 2005, The Guardian newspaper reported that the bid team was demoralized at being “so far behind Paris.” Even bid company staff acknowledged that “the consensus was that we weren’t going to win anyway.”
The bid company spearheaded an impressive marketing campaign and Olympics offer. Despite this, the majority view in the UK remained that the UK would not win. In the final months leading up to the IOC decision, Jowell and the bid company worked tirelessly to increase public support for the Games and developed an even stronger marketing program. In its final lobbying activities, three key points were emphasized by those representing the UK:
The sports experts highlighted the technical merits of the stadium design, which was seen as more sophisticated than Paris’ Stade de France.
Tessa Jowell pledged support from government investment for elite sport and a legacy of investment in school sport and adult participation in sport and physical activity.
Ken Livingstone praised the transformative potential of the Games for London.
All this was sealed with a bit of glamour, with appearances from British Olympics Association chair, Princess Anne, and legendary soccer star David Beckham in the final publicity blitz, with Prime Minister Blair on hand to “press the flesh” of IOC officials in the final hours before the bid-deciding IOC meeting. To cap this, Jowell and Coe agreed that they had to “go for broke” in the presentation to the IOC. “Safe” would deliver the Games to Paris. They therefore decided to showcase, not the corporate sponsors, but 20 young people from East London. They were of more than 10 nationalities speaking 20 languages. Theirs were the faces of modern London.
While the technical plans and marketing campaign might not have convinced the home crowd (or the bookies; the odds were still on Paris the night before the decision was announced), it convinced the people that mattered. The risks paid off, and against all expectations, on 6 July 2005, London was announced as the host of the 2012 Olympics.
The British public were euphoric, and even the institutionally cynical British media had to put a positive spin on the come-from-behind win. Jowell, exhausted by the effort, woke up the next morning saying she “felt the awesome loneliness of leadership.” Weighed down by the huge responsibility that lay ahead even after such a marathon struggle to win the bid, she says the thought crossed her mind that “second place might not have been so bad.” That lasted a moment before her focus shifted to “now we have really got to do it.”
A False Start
Before the Olympics Minister could get home to London, the euphoria turned to catastrophe when four suicide bombers exploded bombs on the London transport system, killing 52 people. All the attention and resources of government were diverted in response to the worst terrorist attack ever on the British mainland. Jowell was given responsibility for government support for the affected families and survivors. This was totally consuming for many weeks after.
To move from bid to staging the biggest ever event in the UK required the establishment of new delivery bodies:
The Olympic Delivery Authority (ODA) as a public body to build the venues;
The London Organising Committee of the Olympic and Paralympic Games (LOCOG) as an independent entity to fund and stage the Games. (See Appendix A for an overview of the Olympic delivery bodies.)
Government also had to establish trading rules in the vicinity of the Games, establish advertising restrictions which would later become the subject of controversy, and ensure the land needed for the Olympic Park was under public control. The London Development Agency (LDA) had started purchasing the site of the Olympic Park earlier in 2003. Work on the Olympic Park started in the summer of 2004, after the existing occupants – including allotment owners, businesses, travelers, and feral cats – were evicted from the site.
Due to the significant pre-planning about governance and legislative plans in the event of a successful UK bid (structures, organizations, and shareholders agreements had all been signed off at the insistence of the bid company to avoid post-bid delays), the London Olympic Games and Paralympic Games Bill was introduced in Parliament just over a week after the announcement that London would host the Games. This speed was a real achievement and radiated confidence.
But while land purchasing, undergrounding power lines, and Games legislation – including the design of and appointments to the Olympic delivery institutions – were well planned and quickly executed, government was less prepared when it came to its own role in the Games. There were disputes about which department would lead on the Games, what civil service capacity existed for a major delivery project, and, crucially, the real size of the budget.
Before the bid was won, Jowell had made clear that, if they won, the budget would have to be reviewed. By the end of 2005, Jowell knew that the actual cost of delivering the Games was going to be substantially higher than the £2.9 billion publicly bandied about before the bid and the final bid number of £4.2 billion. The main reason was that once thorough site inspections were completed and detailed plans developed, it was possible for the first time to calculate the real cost. Security requirements had to be ramped up following the bombing attacks. Throwing fuel on the fire, the Treasury insisted on adding a 60% contingency on the whole project and required the ODA to pay VAT, adding a further £1 billion to the bottom line and pushing the total to £9.2 billion. It took nearly two years to settle the revised budget. According to Jowell, Prime Minister Blair was furious about the Treasury’s deliberate attempt to sabotage the Games. (See Appendix B for a budget timeline.)
The Prime Minister initially refused to accept the new budget number, but eventually told Jowell “to use her own judgment” and left it to her to present and justify the revised budget to the UK parliament. Compounding what Jowell calls a “real moment of crisis,” the media had a field day, panning Jowell’s leadership and the credibility of the effort.
The Treasury initially demanded that it should have sign-off on contracts exceeding £12 million. Jowell says that the Treasury contended it was worried about cost control, but in reality, they were “agents of delay,” aggressively questioning every contract. In a final showdown with the Treasury Committee assigned oversight of the Games, Jowell challenged Committee members to say which of them had ever built a stadium or managed a major sporting event. Of course, none had. Her point well made, Jowell told the Committee she had hired the best people for the job and they should be allowed to get on with their work. She was able to support her stand by showing that up to that point all implementation targets had been met on time and under budget. This included most impressively the undergrounding of the power cables which crossed the site of the Olympic Park.
Government itself had to gear up to oversee what the ODA and LOCOG were doing. The Olympic Park Development was the largest public sector construction project in Europe but compounded by the risk of a fixed deadline for completion.
It did this by creating the Government Olympic Executive (GOE), which Jowell chaired. GOE was purposely designed as a stand-alone unit. As Olympics Minister, Jowell was a passionate advocate, supporter, and broker for the Olympics within government and outside it.
Jowell had hardly secured these victories when Olympic super-skeptic Chancellor Gordon Brown succeeded in his long-time ambition to unseat Prime Minister Blair. Fortunately for Jowell, most of the major agreements were locked in place and implementation was well underway. Brown did not replace Jowell as Olympics Minister, which as incoming Prime Minister had been his prerogative.
The Final Sprint
With stadium construction finally underway in 2008, Jowell was dealt another double blow. Close political ally London Mayor, Ken Livingstone, lost his re-election bid to Conservative Party candidate Boris Johnson. But worse still was the 2008 financial crisis, which saw global stock markets tumble and governments in Europe and the U.S. facing financial catastrophe.
The election of Boris Johnson altered little, mainly because plans were far advanced and London was a major beneficiary. In contrast to the ease of the mayoral transition, the 2008 financial crisis created significant challenges for the project. While most of LOCOG’s sponsorship revenue had been raised prior to the economic downturn,vi the collapse of the private funding of the Olympic Village was seen as the largest budgetary crisis. In May 2009, government made a decision to ramp up the public sector contribution by £350m.vii This proved a sound investment as the Government’s share of the Village was later sold for £570 million.
In the midst of the financial storm and hardly two years before the Games, Jowell’s Labor Party lost the general election to a Conservative-Liberal Party Coalition. Jowell was no longer Olympics Minister. However, Jowell’s foresight in establishing cross-party management of the Games was vital to the stability of the project at this critical stage. The new Minister, with whom Jowell had established an extremely good relationship, had shadowed the Olympics brief since 2004 and throughout this period had unusual access to government briefings on the progress of the Olympics project. He felt “it was a great help to have shadowed the brief for five years” because this, and regular briefings, allowed him to hit the ground running. Jowell says because she had worked hard to build cross-party support, and because the implementation process had been disciplined, turning in projects on time and mostly on budget, the government had little quarrel to pick with what was likely to be a big boost for the national morale at a very difficult economic time.
The new government immediately launched a period of harsh financial austerity to get control of Britain’s extraordinary public debt. While the Olympic budget came under scrutiny, the new Sports Minister recalls that “given the importance of the project, the Olympic budget was largely protected.” Ultimately, only £27 million was taken out of the £9.3 billion funding package for the Olympics, with a totemic decision to remove the publicly funded wrap around the stadium.viii This was subsequently and controversially replaced by a privately tendered wrap, manufactured by Dow Chemicals.
By early 2011, public awareness of and interest in the Olympics started to increase. The public ticket ballot opened in spring 2011 to a flood of interest with 1.9 million people applying for tickets, although many were left disappointed and dissatisfied as they failed to get the tickets they applied for. Jowell’s early insistence that the tickets should be available by ballot and not only with the rich and famous at the top of the queue over time dulled some criticism, but ultimately the ticket applications reached some 24 million, far outstripping availability.
Olympic stadium construction was completed in March 2011, on schedule and over a year ahead of the Games. This was a triumph for ODA, government, and the delivery partner CLM who had met their target date with relative ease.
Now with a year to go, the baton was passed onto LOCOG, thousands of volunteer Games Makers, and operational partners including Transport for London (TfL), the police, the Borders Agency, and the military, who needed to test and prepare the country for Olympics action. The Foreign Office, Defra, and Cabinet Office all had roles to play too – from using the run-up to the Olympics for diplomatic opportunities to ensuring vets were on hand for animals used in the opening ceremony. (See Appendix C for the scale of public sector activities.)
A series of Home Office-led test exercises with police, military, and emergency workers took place to ensure security and other operational concerns were ready for the Games and that “everyone was in the right frame of mind.”ix These exercises included “Exercise Forward Defensive” – a February 2012 two-day exercise involving 2,500 people simulating a response to a bomb on the Tube networkx and “Exercise Olympic Guardian,” which took place over eight days in May 2012 and included the deployment of fighter jets, helicopters, and ships around London and Weymouth.xi The final test exercises neatly transitioned into the operational phase of the Games, which officially began on 19 May 2012 when the Olympic Torch Relay began.
As the Games approached, TfL, the Department for Transport (DfT), and LOCOG were working to prepare Londoners and their transport system for the estimated 20 million extra journeys that would take place during the Games. The major public information campaign encouraging individuals to plan their travel during the Games started on 30 January 2012.xii Prior to this, organizations involved in delivering public transport during the Games had started working with businesses in November 2010 through the “Travel Demand Management Business Influencer Campaign,” urging businesses to plan for the impact of the Games. The Department for Transport led a cross-government initiative to reduce travel into central London with 17 government departments committing to change at least 50% of their own travel footprint over summer 2012. A trial week for this programme called “Operation Step Change” took place in spring 2012. Testing of the Olympic travel programme continued into July 2012, with commuters being deterred from central London through delays caused by the testing.xiii Overall this was a successful programme, with up to 35% of people adapting their normal travel behaviour to take account of the Olympics.
The role of LOCOG during this period should not be underestimated. They took control of the Olympic Park in January 2012, at which point large quantities of work in order to make venues Games-ready still needed to be undertaken. They received considerable assistance from the ODA with this. In addition to the work on venue preparation, they organised the Torch Relay, which confounded expectations and was viewed by an estimated 12 million people as it made its journey around the UK.xv LOCOG also had key roles to play in areas including venue security, transport management, and the monumental task of training and working with thousands of volunteer Games Makers, another runaway Games success story. Although TfL were responsible for running London’s public transport system, LOCOG’s role included assisting with the development of the Olympic Route Network and working with transport partners on delivering the public transport system. Similarly, although the Home Office was ultimately responsible for delivering security arrangements around the Olympic Games, LOCOG were responsible for contracting for security arrangements at the Olympic venues and playing an increasingly leading role in discussions around security in the run-up to the Olympics.
Overall this went remarkably smooth, with the very serious exception of G4S failing to fulfill their contract to deliver a full complement of guards for venue security. This was a major hiccup in the last weeks before the Games and was subject to intense media scrutiny. In the event, the detailed contingency planning that government had undertaken in collaboration with LOCOG moved into action quickly though, and the armed forces were deployed to fill a 3,500-person shortfall. This was not the disaster it could have been, as a senior civil servant at Cabinet Office recounted: “the plan was exactly as it was, just with more highly trained and disciplined personnel providing the security.”
As the end of July drew close, eyes now turned to the Olympics themselves. The torch relay had built a mounting enthusiasm for the Games and only weeks before the Opening Ceremony, UK Sport confirmed they were aiming for Team GB to finish in the top four of the medals table with a medal take of at least 48 medals.
Finally the Flame is Lit
A decade after Jowell embraced the idea that London should host the 2012 Olympics, she watched the Olympic torch lit in the spectacular main Olympic arena. What followed were the most successful Games in Olympic history. Jowell, through determined and unrelenting leadership, had succeeded against enormous political, economic, and organizational odds. In retrospect, Jowell says she thinks success at the end of the day was because the effort reflected the “values and the mood of the time.”
Jowell says the project had been very sensitive to local communities affected by the Olympics infrastructure development, they kept costs under control, and the entire process had been transparently conducted. Jowell also takes pride in the fact that not a single life was lost nor any serious injury occurred in the construction of the Olympic venues.
Despite initial reticence, the British public enthusiastically embraced the project because many communities beyond the city of London had seen benefits from the build-up to the Games, but also because the nation desperately needed a morale boost as it wrestled with the worst economic crisis in a century. In retrospect, Jowell says that the most troubling part of the process was the time it took to come up with a reliable cost estimate. The Olympic bid process makes this almost impossible and the eventual budget contained large provisions, VAT, a doubled security budget post-London bombings, and a programme contingency of 60% that could not have been foreseen three years before the decision to award the Games to London. Sometimes, as a leader, you just have to be prepared to take the beating!
Questions for Discussion
How did Jowell continue to focus on her priorities in spite of the recurring distractions?
How did Jowell manage the politics, including the relationship with the PM and the Chancellor of the Exchequer?
How did Jowell ensure continuity of her goal through a change of government?
How did Jowell secure the right financial support to deliver on her mission?
What did Jowell do to build a strong and effective team?
Appendix
Appendix A: The Olympic Delivery Bodies
LOCOG and the ODA both sat outside of government, but were hugely different organizations. The ODA – as a statutory executive NDPB – existed in a structure with which DCMS was familiar. The London Olympic and Paralympic Games Act 2006 gave the ODA broad powers, including the right to “take any action that it thinks necessary or expedient for the purpose of preparing for the London Olympics.” The Secretary of State for Culture, Media and Sport had responsibility for appointing the ODA Board, the first ODA chief executive, and had the right of veto over appointees to be finance director, transport director, or any chief executive other than the initial appointee.
LOCOG was an entirely different entity. Its structure had been agreed during the bid phase, meeting the requirement of the Olympic Charter that it report directly to the IOC Executive Board. It was clear from interviews that while LOCOG viewed its relationship with government as important, its crucial relationship was with the IOC. LOCOG was accountable to its three stakeholders – the Secretary of State, the Mayor of London, and the British Olympic Association – who were collectively responsible for appointing the Board under the terms of a joint venture agreement. As a private company limited by guarantee, however, it did not see itself as having a conventional “sponsorship” relationship with government. This was heightened by its determination to remain financially independent of government, raising its £2bn budget from the private sector and IOC (while government would put close to £1bn into LOCOG, this was largely to cover scope transferred to LOCOG, rather than for its core functions).
Appendix B: The Budget Timeline – Key Events
May 2003: Government and Mayor of London agree memorandum of understanding providing a public sector funding package (PSFP) of £2.375bn to meet the costs of the Games – £1.5bn of which would come from the National Lottery. Government also commits a further £1.044bn of Exchequer funding for non-Olympic infrastructure. Combined with anticipated private sector funding of £738m, the expected gross cost of the Games was £4.036bn (excluding the LOCOG budget).
31 October 2005: Olympic cost review steering group (an officer-level group initiated to review all costs associated with the London Olympic Games) meets for the first time.
21 November 2006: Tessa Jowell indicates to the House of Commons Culture, Media and Sport Select Committee that additions to the Olympic budget in the bid will include an additional £400m to be spent on the ODA’s delivery partner, and £900m in the costs of the Olympic Park. Further liabilities are identified as the tax status of the ODA, the need to develop a programme contingency, and increased security costs.
15 March 2007: Revised PSFP announced, including ODA budget of £5.254bn, an ODA tax bill of £836m, a £2.247bn programme contingency and revised policing and wider security costs of £600m, up from £190m at the time of the bid.
November 2007: Announcement of ODA baseline budget at £6.09bn, which served as a basis for future reporting.
13 May 2009: Public sector funding is agreed for the construction of the Olympic Village after a potential public-private deal collapses.
24 May 2010: PSFP is reduced to £9.298bn.
20 October 2010: PSFP is not reduced in the Comprehensive Spending Review; the publicly funded “wrap” around the stadium is removed, saving £7m from within the PSFP.xvi Dow Chemical won a competitive tendering process to privately fund a wrap around the stadium in August 2011. PSFP funding is shifted from construction to operations.
12 August 2011: Majority of the Olympic Village and adjoining land is sold to Qatar’s investment arm for £557m.
6 December 2011: DCMS and National Audit Office both report that venue security costs have risen to £553m – an increase of £271m from October 2010. The NAO also puts the cost of 18 legacy programmes at £826m, with this cost sitting outside the PSFP for the Games. £41m of public money is put into LOCOG to fund more ambitious opening and closing ceremonies for the Olympics and Paralympics, with a total of £354m of uncommitted programme contingency remaining.
31 October 2012: Final GOE quarterly financial update is released. The anticipated final spend against the PSFP is £8.921bn – a £377m saving. Estimated costs of policing and venue security respectively are £455m and £514m – a combined decrease of £60m against expectations in May 2012.
14 November 2012: LOCOG release details of their revenue streams to the Greater London Assembly, showing that their upper sponsorship target of £700m has been exceeded by £46m.
Appendix C: Public Sector Scale
11 hospitals designed as “Olympic hospitals” on standby to provide free medical care for the “Olympic Family”.xvii
52 police forces involved in providing security for the Olympics – every police force in the country.
98% of scheduled kilometres run on schedule on the Tube, London Overground, and London bus network during the Olympics.
200 extra buses provided in London for the Games.
4,000 extra Games-time train services provided over the Olympics and Paralympics.xviii
13,000 London businesses attended seminars prior to the Olympics where TfL explained Games transport impacts.
15,000 police officers deployed on the Olympic operation on peak days.xix
18,200 troops required to provide security for the Olympics at peak timesxx – nearly double the number serving in Afghanistan at the time.xxi This number consisted of 13,500 service personnel announced in December 2011, a further 3,500 deployed as assurance against G4S’ failure to meet their contract on July 12, 2012,xxii and an additional contingency of 1,200 troops called up on July 24.xxiii
138,000 passengers handled by Heathrow on the busiest days of the Olympics – up 45% on normal levels.xxiv
450,000 people requiring some level of special access for the Games who were background-checked by the UK Border Agency (UKBA), including contractors, “Olympic Family” members, and volunteers.xxv
3,000,000 additional public transport trips above normal levels on the busiest day of the Games in London.xxvi
References
Where relevant throughout this report references to the success of the ‘Olympics’ should be taken as applying to the success of the 2012 Olympic & Paralympic Games.
House of Commons Culture, Media and Sport Select Committee, A London Olympic Bid for 2012 (2003), p. 11
House of Commons Culture, Media and Sport Select Committee, A London Olympic Bid for 2012 (2003), p. 16
Mihir Bose, “Olympics: Jowell seeking to win over skeptics,” The Telegraph, January 29, 2013, link
Mike Lee, The Race for the 2012 Olympics (2006), p.14
Roger Blitz, “Rogge hits back over sponsorship criticism,” Financial Time, July 9, 2012, link
Owen Gibson, “Olympic Village to be fully funded by taxpayers,” The Guardian, May 13, 2009, link
ODA, 2011/12 Annual Report
“London 2012: Olympics and Paralympics security test,” BBC News, February 22, 2012, link
“London 2012: Major Olympic security test unveiled,” BBC News, April 30, 2012, link
House of Commons Transportation Committee, Section 3.5 from Session 2010-12 on Transport and the Olympics, March 14, 2012, link
Sam Jones, Paul Owen, and Haroon Siddique, “Olympic test-run on London transport leaves commuters grumbling,” The Guardian, July 10, 2012, link
Simon Israel, “New security challenges for Paralympic torch relay,” Channel 4 News, August 20, 2012, link
“Scrapping London 2012 curtain ‘sensible’, Lord Coe says,” BBC News, November 2, 2010, link
London 2012 Olympic Games healthcare guide
Network Rail, Our Plans for London 2012
House of Commons Home Affairs Committee, Olympics Security (2012)
David Horsey, “U.K. military at Olympics outnumber U.K. troops in Afghanistan,” Los Angeles Times, July 27, 2012, link
Hansard HC Deb 12 July 2012, vol 548, col 451
House of Commons Home Affairs Committee, Olympics Security [OS 07] (2012)
Heathrow Airport, Heathrow’s Preparations for the London 2012 Olympic and Paralympic Games
UKBA 2011/12 Annual Report
TfL, Hosting a Great Games and Keeping London Moving this Summer
South Africa has one of the highest HIV/AIDS prevalence rates in the world. The country’s response to the epidemic for a period of about eight years was hampered by misguided political leadership questioning the causality of HIV/AIDS and the effectiveness of antiretroviral therapy. This situation was finally reversed in 2009 when President Jacob Zuma was elected. This case study outlines the problem, changes and outcomes of South Africa’s HIV/AIDS policy reform as follows:
South Africa’s response to its HIV/AIDS epidemic was impeded by nearly two decades of poorly informed policy, particularly under the leadership of Thabo Mbeki; believing that HIV did not cause AIDS, claiming that it was linked to social factors, and giving preference to the use of Virodene, a drug found to be highly toxic, instead of ARVs.
As a result of these policies, the country had an adult HIV/AIDS prevalence rate of 17.3% in 2011. There were 310,000 AIDS related deaths that year and 1.9 million orphans due to the AIDS deaths. There was also a high mother-to-child transmission rate because of restricted use of freely donated nevirapine, which prevents mother-to-child transmission.
The election of Jacob Zuma in 2008 ushered in a dramatic shift in the country’s HIV/AIDS policy. He and Minister of Health, Aaron Motsoaledi, quickly implemented plans for countrywide prevention and testing, and providing ARV treatment without charge through public facilities to all who require it.
Minister Motsoaledi introduced the HIV and AIDS Counseling and Testing Campaign in 2010 with the aim of regular HIV testing and counseling, promoting behavior change and regular condom use, providing voluntary medical male medical circumcision, scaling up syndromic management of STI and intensified prevention of mother-to-child transmission programs. Also implemented task shifting to increase the number of professionals able to test for HIV, prescribe ARVs, and administer ARV treatment.
As a result of the newly implemented strategy, 20 million South Africans have been tested for HIV/AIDS over the past 3 years; mother-to-child HIV transmission has decreased; life expectancy has risen; over 600,000 men have voluntarily been circumcised; the number of facilities providing ARV treatment increased significantly, as had the number of patients receiving ARV treatment; and expenditure on combating HIV/AIDS in South Africa is now the highest of any middle-income or low-income country.
On taking office in 2009, Minister Aaron Motsoaledi was faced with an immediate political priority. Reversal of the existing HIV/AIDS policy had been a part of President Zuma’s election platform and there was huge domestic and international pressure for a quick change. Minister Motsoaledi tackled the challenge with energy and skill quickly convincing the South African public and the international community that the new government’s commitment was genuine and rapidly launching highly publicized efforts to expand prevention and treatment programs. Minister Motsoaledi’s efforts have transformed South Africa’s HIV/AIDS management program from an international moral outrage into a global example.
HIV/AIDS Policy Reform in South Africa – The Transformation after 2009
South Africa is one of the countries worst affected by HIV/AIDS. Historically, the HIV/AIDS response in South Africa was impeded by political leaders who questioned the science behind the causality of HIV/AIDS and the effectiveness of ARVs. However, since 2008, under the leadership of President Jacob Zuma and Minister of Health Dr. Aaron Motsoaledi, South African HIV/AIDS policy changed radically, establishing national-scale HIV prevention programs and the world’s largest AIDS treatment effort leading to a five-year gain in national life-expectancy.
In 2011, among South African adults aged 15–49, 17.3% were HIV-positive, more than triple the rate for the whole of sub-Saharan Africa (5.2%) and a global adult prevalence rate of 0.8%. Black South Africans, who make up four-fifths of the country’s population, have been the hardest hit: 13% of their total of all ages are HIV-positive, compared with 3% of coloreds and Indians and just 1% of whites. Even though HIV prevalence is 17.3% among the general population, it varies a lot by region. In KwaZulu-Natal, the region with the highest prevalence, just under 40% of 15–49 year-olds are living with HIV. Furthermore, there were 310,000 related deaths and 1,900,000 orphans due to AIDS. In addition, a characteristic of AIDS in South Africa is the close link with the prevalence of tuberculosis. Current HIV/TB co-infection rates exceed 70%, with TB being the most common opportunistic infection among them. Due to late detection, poor treatment, management and failure to retain TB patients on treatment, drug-resistant forms of TB (DR-TB) have increased significantly.
The South African government’s initial response to the epidemic was significantly lacking due to poor political leadership, AIDS denialism and failure to provide comprehensive AIDS treatment and prevention programs. This situation led to large-scale protest by civil society in South Africa and from the international community. By 2008 the government recognized the need to change course. This policy sea change did not gather full momentum until the election of President Jacob Zuma in May 2009 and the appointment of Minister of Health Dr. Aaron Motsoaledi. Over the past three years, South Africa has become a model for comprehensive HIV/AIDS management.
Background
The first attempt to formulate a post-apartheid response to AIDS in South Africa began with the launch of the National AIDS Committee of South Africa (NACOSA) in 1992 following consultations between the African National Congress (ANC), the National Party government and civil organizations. This in turn led to the National AIDS Plan in 1994. Since then, the government’s policy evolved to formulating the HIV/AIDS and Sexually Transmitted Disease Program in 1996; the establishment of the South African National AIDS Council in 2000; and, in the same year, the compilation of the country’s comprehensive National HIV/AIDS and STI Strategic Plan for 2000–2005. Despite all these initiatives, there was barely any progress in the HIV/AIDS response. This can be attributed to a history of prevarication of HIV/AIDS by top political leadership.
In 1996, Deputy President Thabo Mbeki, under President Nelson Mandela, was a major actor in the Virodene saga, a significant event in South Africa’s HIV/AIDS history. At the time, a group of academics of the University of Pretoria claimed they had found the cure for AIDS through a vaccine called Virodene, a drug the Medicines Control Council warned was dangerous and toxic. Mbeki, a staunch supporter of “Africans finding African solutions,” became the chief champion of Virodene. He thought it would be the perfect platform from which to launch his vision of an African Renaissance, led by South Africa. Tests by independent scientists, however, found Virodene could be highly toxic and could cause severe liver damage. In 1999, Mbeki was elected President of South Africa and in his first address to the nation, Mbeki declared HIV/AIDS “everyone’s problem” and emphasized how the country needed to face AIDS to save the youth, its education and the country’s economy.
After his initial unambivalent stance, Mbeki’s approach changed dramatically by June 1999 when he declared his support for the view that HIV does not cause AIDS. Throughout his nine-year tenure as South Africa’s President, Mbeki aligned his views with what have been termed “dissident” scientists, a group of scientists who denied the conventional theory that the HIV virus caused AIDS and that antiretroviral drugs could save the people who tested positive for it. During this period Mbeki began to argue that HIV and AIDS were linked to social factors such as poverty, malnutrition and poor health care. Mbeki stubbornly continued to embrace this position even as the evidence against it became overwhelming. While Botswana and Namibia, South Africa’s neighbors, provided antiretrovirals to the majority of their citizens infected by HIV, South Africa under Mbeki failed to do so. President Mbeki also restricted the use of freely donated nevirapine in the prevention of mother-to-child transmission of HIV.
As a result, ARVs were unavailable to patients in state clinics and hospitals, whether rape survivors or health care workers who had accidentally been exposed to the virus. The impact of this policy was severe, both in terms of avoidable loss of life and the long-term damage to HIV/AIDS education efforts in South Africa. The only state-funded HIV/AIDS program was the provision of ARVs to pregnant women for Preventing Mother to Child Transmission (PMTCT). From the late 1990s, a series of protests and marches driven by civil society and religious groupings led to a Constitutional Court challenge to oblige the government to provide ART to HIV-positive mothers in an effort to prevent mother-to-child transmission. In July 2002 the Constitutional Court ruled that the government had a constitutional duty to provide AIDS drugs to pregnant women to prevent transmission of HIV to their babies. The Government was forced to comply with the Court ruling, but there was no change in general HIV/AIDS policy by the Mbeki administration.
By the time President Mbeki left office in September 2008, studies estimate that upwards of 330,000 AIDS-related deaths could potentially be attributed to Mbeki’s recalcitrance on HIV/AIDS. In addition, an estimated 35,000 babies were born with HIV by not implementing a mother-to-child transmission prophylaxis program using nevirapine before being compelled to by the Constitutional Court.
While South Africa has a sophisticated infrastructure, a well-developed private sector and a stable macro-economy, the high prevalence of HIV/AIDS partly explains why South Africa has not achieved some targets for MDGs related to outcomes such as employment, income levels, and life expectancy. Realizing the severity of the HIV/AIDS pandemic as a local and global health emergency as well as a development emergency, the new South African government of Jacob Zuma elected in May 2009 and Minister of Health Aaron Motsoaledi moved quickly to implement effective measures to combat the epidemic.
Situation Analysis
Minister Motsoaledi brought strong leadership and high energy to his position. He quickly won over civil society and re-energized the public health sector. Minister Motsoaledi’s fervor for improving service delivery has uncovered the inefficiency of how health facilities and programs had been run prior to his coming to office—from the administration level and service delivery to the supply of essentials. Considering HIV/AIDS, he quickly put in motion programs for countrywide prevention, detection and immediate treatment with ARVs for all the people who tested HIV positive. In the first year of his tenure, Minister Motsoaledi was tireless in his efforts to mobilize all sectors of society in support of a dramatically ramped up national campaign to prevent and treat HIV/AIDS. Most notably, Minister Motsoaledi’s passion mobilized other key political leaders, and with the support of President Zuma, also mobilized the public to take up the campaign against HIV/AIDS. It was not long before local and international studies referred to the revolution Minister Motsoaledi had brought about in health in South Africa, especially in HIV/AIDS.
Strategy
The fight against HIV/AIDS has been a major focus for Minister Motsoaledi from the beginning of his appointment. The cornerstone of the new strategy to combat HIV/AIDS was the HIV and AIDS Counseling and Testing (HCT) Campaign, launched in 2010. The HCT campaign aimed to scale up the integrated prevention strategy based on: regular HIV testing and counseling, promoting behavior change and condom usage, providing medical male circumcision, scaling up syndromic management of STI and intensified prevention of mother-to-child transmission (PMTCT) programs. Another aim of the HCT Campaign is that people should know their status early. This was done by massively scaling up HCT services in public and private facilities, homes, workplaces and public spaces, followed by the administration of ARVs. Some 500,000 people were tested for HIV in the first six months of the HCT campaign. According to statistics on the HCT campaign, 65% of the people who participate and want to know their HIV status are women, 5% are children and only 35% are men. Minister Motsoaledi also announced that comprehensive reproductive health education would be introduced in government schools, including family planning and sexuality education, HIV counseling and testing should be happening in schools.
Scientific evidence showing that male circumcision reduces the risk of sexual transmission of HIV from women to men by 60% prompted the South African government to include voluntary medical male circumcision (VMMC) as an integral part of its HCT campaign. As such, the campaign offers all men aged 15–49 voluntary medical circumcision at public health facilities. In April 2010, KwaZulu-Natal became the first province to offer VMMC services at public clinics, a region where male circumcision is not traditional. The scale-up of VMMC to all nine provinces has meant that South Africa (along with Kenya and Zambia) ranked one of the highest globally, in terms of number of circumcisions performed. In 2009, 9,168 men were circumcised and in 2010 this increased to 121,117 and subsequently to 347,973 in 2011.
The impact of HIV/AIDS on children has been vast as well, but since 2009 South Africa has had one of the sharpest declines in new infections among children. In 2011, more than 95% of pregnant women with HIV received treatment to prevent the infection of their child. Yearly infections in children have dropped from 56,500 in 2009 to 29,100 in 2011. In 2009, around 30% of pregnant women were HIV positive, demonstrating the need for South Africa to deliver effective PMTCT programs. South African guidelines for PMTCT issued in 2008 were heavily criticized for not meeting World Health Organization recommendations. In 2010 South Africa released new PMTCT guidelines, more in line with WHO recommendations. In South Africa’s guidelines HIV-positive pregnant women are advised to start treatment when their CD4 count drops below 350 cells/mm³; all pregnant women who test HIV-positive will begin receiving treatment at 14 weeks rather than in the last term of pregnancy. In addition, HIV-positive women are advised to receive antiretroviral drugs postpartum. The latest National Strategic Plan aims to reduce MTCT to less than 2% at six weeks after birth and less than 5% at 18 months by 2016.
In addition, in May 2010, South Africa implemented task shifting. Under task-shifting, nurses, rather than doctors, can initiate antiretroviral therapy; lay counselors, rather than nurses, can carry out HIV tests, as well as provide support for orphans usually done by social workers; and pharmacy assistants, rather than pharmacists themselves, can prescribe ARV drugs. It is believed task shifting vastly increases the access points to treatment and care by reducing the ‘bottlenecks’ in the system created by a lack of staff able to perform certain tasks. Minister Motsoaledi approved the new regulations, which allow a person who is not a healthcare provider (such as a counselor who has received training in taking blood) to do so. In 2011 it was announced that the number of nurses trained to administer ARVs has increased from only 250 nurses in early 2010 to 2,000 nurses in May 2011.
The commitment of the current government and Minister Motsoaledi is further demonstrated through a new National Strategic Plan on HIV/AIDS and TB for the period 2012–2016. This Strategic Plan will integrate HIV and AIDS and TB in the same strategic plan and will outline a 20-year vision of the country in the fight against the double scourges of HIV/AIDS and TB.
Outcomes
According to government statistics, 20 million South Africans have been tested for HIV/AIDS since the HCT campaign was launched in April 2010, exceeding the target of 15 million.
The rate of mother-to-child HIV transmission at 6 weeks has been reduced from 8% in 2008 to 3.5% in 2010 and down to 2.7% in 2011. The latest National Strategic Plan aims to reduce MTCT to less than 2% at six weeks after birth and less than 5% at 18 months by 2016.
Life expectancy has risen from 56.5 years in 2009 to 60 years in 2012.
The medical male circumcision program is under way and is doing very well. South Africa has circumcised 600,000 people who were not circumcised before the program was launched. The number of circumcisions performed in 2010 placed South Africa among the highest globally, along with Kenya and Zambia. The province of KwaZulu-Natal is aiming to circumcise at least two million males by 2015.
There were only 490 ARV treatment sites in February 2010. By the end of 2012, this number increased to 3,000 facilities, which were well equipped to initiate ARV treatment. It was estimated that 1.7 million people were on ARVs in 2012 compared to approximately 920,000 in 2009, an approximate 75% increase in just 2 years. The State is hoping that by 2015, the number of people on treatment will reach 2.5 million. The ARVs have been called the ‘Lazarus drug’ because people rise up and walk.
Table 1: Temporal trends in the HIV and tuberculosis epidemics in South Africa
2006
2007
2008
2009
2010
2011
HIV/AIDS indicators
People living with HIV (million)
4·99
5·27
5·13
5·35
5·47
5·58
Antenatal HIV frequency (%)
29·1%
29·4%
29·3%
29·4%
30·2%
NA
HIV frequency in the total population (%)24
10·2%
10·2%
10·6%25
10·4%26
10·5%26
10·6%
Male condoms distributed (million)
376
45326
28426
44526
49226
347
Female condoms distributed (million)
3·6
3·326
4·326
3·626
5·026
6·4
Adult medical male circumcisions25,27
NA
NA
5190
9168
121117
347973
Adults and children receiving antiretroviral therapy28
235000
382000
588000
912000
1287000
1793000
Antiretroviral coverage (%)29
19%
28%
35%
51%†/29%†
64%†/39%†
79%†/52%†
Deaths due to HIV/AIDS (%)
52·3%
51·2%
49·2%
46·4%
44·3%
43·6%
Tuberculosis indicators
Prevalence (all forms; per 100 000 people)30
797
789
792
809
795
NA
Estimated incidence (all forms; per 100 000 population)30
940
948
960
971
981
NA
Estimated number of incident cases (all forms)
450000
460000
470000
480000
490000
NA
Case detection (%)30
67%
68%
73%
75%
72%
NA
Treatment success of new smear positive cases (%)30,31
74%
74%
76%
73%
73%
80%
Death rate (per 100 000 population)30
57
53
51
52
50
NA
Patients with HIV co-infection (%)30
59%
59%
59%
58%
60%
65%
NA = not available. *Eligible when CD4 <200 cells per μL. †Eligible when CD4 <350 cells per μL.
References
Auvert B, Taijaard D, Lagarde E, Sobngwi-Tambekou J, Sitta R, Puren A. Randomized Controlled Intervention Trial of Male Circumcision for Reduction of HIV Infection Risk: The ANRS 1265 Trial. PLoS Medicine. 2005; 2(11). http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1262556/