
Executive Summary
“If the agricultural sector does not invest enough, the cases end up in the hospital and the burden goes to the health sector to treat malnutrition”
Dr. Kesetebirhan Admasu served as Minister of Health of Ethiopia from 2012 to 2016. Upon entering office, Ethiopia had been making progress toward reducing stunting from 67% in 1992 to 44% in 2011, but significant rural-urban and regional variations meant that malnutrition persisted as one of the leading causes of infant and child mortality.
The Government of Ethiopia had already begun on a path towards heavy investment in nutrition including the reduction in stunting, wasting, anemia, and dietary diversity outcomes, beginning with the establishment of the National Nutrition Program I (NNP I, 2008-2015). Further recognizing the importance of nutrition as a pillar for human capital development and economic growth, Minister Admasu, along with Deputy Prime Minister, H.E. Demeke Mekonnen, launched the Seqota Declaration in July 2015, a high-level commitment by the Ethiopian government to end stunting in children under two years by 2030. Minister Admasu knew that incorporating nutrition goals and actions into existing programs across sectors could enhance their nutrition sensitivity and thus their likelihood of improving nutrition outcomes. Thus, the Declaration was accompanied by the launch of the National Nutrition Program II (NNP II, 2016-2020) and the National Nutrition-Sensitive Agriculture Strategy (2016-2020).
The causes and consequences of suboptimal nutrition span many sectors (such as agriculture and health) and thus the improvement of nutrition outcomes necessitates multisectoral coordination. Despite their expressed interest, policymakers struggle to create sustainable multisector policies and continue to address these issues in a siloed fashion, missing the opportunity to create even greater outcomes from the integration of these spheres. This case study will examine the Seqota Declaration to show how Ethiopia has made nutrition a national and inter-ministerial political priority, enabled consensus-building across sectors, and established coordinating bodies at the national and regional levels to implement.
NNP I: Preliminary Efforts towards Intersectoral Collaboration
Agriculture, health, and nutrition are mutually reinforcing sectors. Agriculture constitutes 40% of Ethiopia’s GDP and 80% of exports, and 75% of Ethiopians’ livelihoods depend on rain-fed agriculture. While agriculture and health are often administered as disparate entities, nutrition serves as the link between these two, with dietary intake closing the value chain from agricultural productivity to improved health outcomes. As part of this more multisectoral approach, the sector has shifted from purely nutrition-specific interventions, such as exclusive breastfeeding and optimal complementary feeding, to include nutrition-sensitive interventions, such as water, sanitation, and hygiene, and food fortification.
The NNP I that Minister Admasu inherited was focused on “immediate causes of suboptimal growth and development” and the effects of nutrition programs on malnutrition. In particular, there was a focus on integration and coordination across nutrition-specific interventions that were supported by “evidence-enhanced decision making.” Nutrition programs were scaled up and an implementation platform was created in the form of the National Nutrition Coordinating Body (NNCB) and the National Nutrition Technical Committee (NNTC).
The NNCB involves 13 government sectors and is primarily led by the Minister of Health, with the Ministers of Agriculture and Education as co-chairs. It meets every six months and develops an annual work plan to ensure that various sectors are mainstreaming nutrition activities into detailed sector-specific plans, allocating budget to nutrition interventions, and assigning focal persons to work on nutrition. The NNTC, which also involves 13 government sectors and nongovernmental stakeholders, has three steering committees on program management, food fortification, and monitoring and evaluation. In addition to the NNCB, the Ethiopian government established Regional Nutrition Coordinating Bodies (RNCB) in most regions, as well as coordinating bodies at the woreda level.
Nutrition interventions under NNP I were intended to cut across sectors through the “Nutrition-Sensitive Agriculture Strategy, National Food Security Strategy, National Health Sector Transformation Plan, National Food Fortification, and the National School Health and Nutrition Strategy.” This multisectoral coordination was able to demonstrate some improvement in outcomes but was not fully effective in creating the intended outcomes.
The Seqota Declaration: Interministerial Support for Transformational Change
Improving nutrition to achieve sustainable development was the core vision of the Ethiopian government. However, it could not be done using traditional methods and did not pertain to only one sector. There was a need to tackle the issue from several angles by engaging different sectors in order to deliver high impact nutrition-specific, nutrition-sensitive, and infrastructure-smart interventions. Thus, the Seqota Declaration was unveiled by the Ethiopian government, led by Minister Admasu, in July 2015 to end stunting in children under two years by 2030. The Seqota Declaration builds on and supports the implementation of NNP II which highlights the “Five Building Blocks of Effective Nutrition Governance” as consensus building and coordination, political commitment, financing, service delivery capacity, and transparency and accountability.
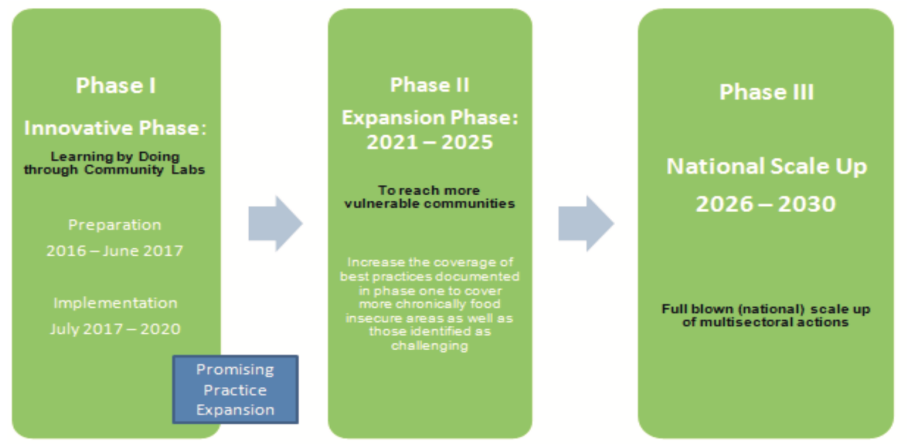
Due to its ambitious nature, the Seqota Declaration Implementation Plan is divided into three distinct phases (Figure 1) to be executed over a 15-year period. Although they each have different specific goals, they are all part of a bigger picture, which intends to promote and ensure a smooth transition/path to success. During the innovation phase (2016-2020), new and innovative ideas are being tested out in order to generate evidence for interventions, while the expansion phase (2021-2025) involves increasing the coverage of the lessons learned from the innovation phase to reach more vulnerable communities. Finally, the scale-up phase (2026-2030) will involve national scale-up throughout the country. The innovation phase is being implemented in 33 select woredas (districts) in Amhara and Tigray regions where stunting prevalence is high and over 4 million people are entirely dependent on rain-fed agriculture and animal husbandry.
Figure 1. The Three Phases of the Seqota Declaration
The Seqota Declaration has ten multisectoral strategic objectives as outlined below and is implemented by six federal sectors (Ministry of Health; Ministry of Agriculture; Ministry of Water, Irrigation and Energy; Minister of Labor and Social Affairs; Ministry of Education; Ministry of Women, Youth, and Children). In addition to these six ministries, development partners and community organizations are also involved.
Strategic Objectives of the Seqota Declaration
- Improve the health and nutritional status of adolescents, women, and children.
- Ensure 100% access to adequate food all year round.
- Transform smallholder productivity and income.
- Ensure zero post-harvest food loss.
- Enhance innovation around the promotion of sustainable food systems (climate-smart).
- Ensure universal access to water supply, sanitation, and adoption of good hygiene practices.
- Improve the health and nutrition status of school children.
- Improve the nutritional status of pregnant and lactating women and children through PSNP interventions.
- Improve gender equity, women’s empowerment, and child protection.
- Improve multi-sectoral coordination and capacity.
Interministerial Collaboration in Practice
The Seqota Declaration has only recently been implemented and is still in its preliminary innovation phase. Thus, it is not yet known if Ethiopia will reach its goal of reducing stunting among children under two by 2030. However, there is still much to be learned from its ambitious approach to harnessing the efforts of six different ministries to address one significant challenge. This section will highlight certain elements of inter-ministerial collaboration that have been put into practice in Ethiopia as part of its journey towards achieving the Seqota Declaration.
Demonstrating Political Leadership and Commitment
The bold ambition of the Seqota Declaration would never have occurred without strong political leadership and commitment. However, equally important was the consultative process that was used to inclusively develop the Declaration and create local ownership and buy-in. At the federal level, this commitment to making the Seqota Declaration a priority could be seen through the political capital spent by the Deputy Prime Minister to get the commitment of the two Regional Presidents of Amhara and Tigray. At the regional level, this leadership commitment could be seen through the financial investment made towards the Declaration, at an amount which was higher than that of the federal government. This latter shows the deep interest of the Regional Presidents for the successful implementation of the initiative in their respective regions.
Both governmental and non-governmental officials highlighted four salient drivers of this political prioritization and movement toward nutrition-related multisectoral collaboration:
- The international community’s emphasis on reducing undernutrition, specifically the MDGs, SDGs, and increased donor funding towards these priorities.
- The 2012 Cost of Hunger in Africa study which showed that 16.5% of Ethiopia’s GDP was lost to child undernutrition through healthcare costs, loss in education, and workforce absenteeism.
- Field trips to learn from the experiences of other countries, particularly Brazil and Israel, at implementing inter-ministerial nutrition strategies.
- Nutrition champions within Ethiopia like Minister Admasu, the Minister of Agriculture, and former first lady H.E. Roman Tesfaye.
For an initiative as ambitious as the Seqota Declaration, leadership commitment is key. The political leadership exhibited by the federal government through the consultative process at all levels facilitated local ownership of the Seqota Declaration. This latter has resulted in the Seqota Declaration becoming a higher priority for leaders at both the federal and regional levels. The meeting between the Deputy Prime Minister and African Development Bank president to mobilize more resources for the initiative.
Identifying Relevant Actors and Roles
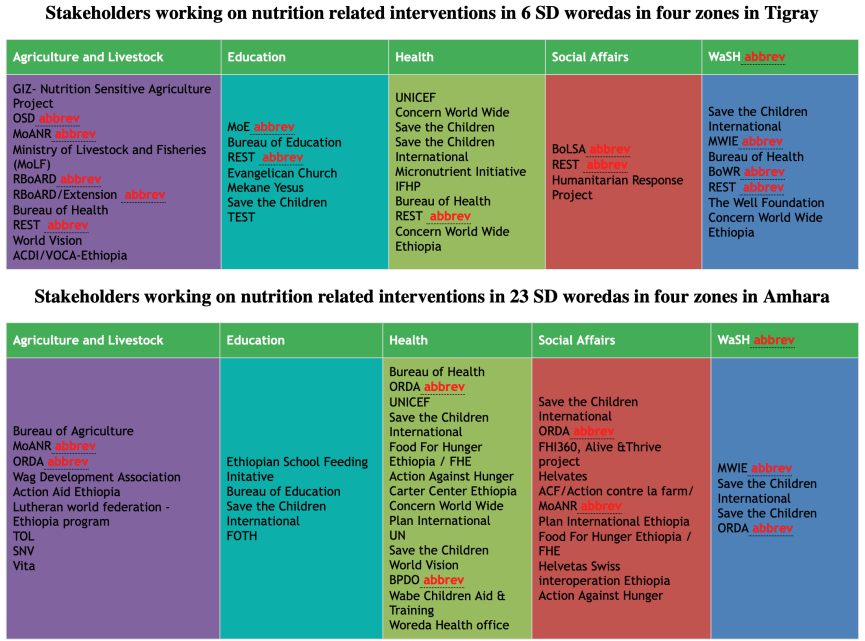
Stakeholder mapping was a critical first step to effective collaboration both internally and with external government partners. It is impossible to mobilize and utilize all actors towards a common goal in a complementary fashion without knowing who they are and what they can do. Thus, the implementation of the Declaration began with a stakeholder mapping exercise to understand which actors were at play across various sectors. Figure 3 outlines the results of the stakeholder mapping exercises conducted in Tigray and Amhara.
Figure 3. Stakeholders Mapping in both regions (Tigray and Amhara).
Clearly Defining Collaboration in Context
Minister Admasu noted that in the past, “interventions in agriculture, health, and other sectors were not properly contextualized” and that everyone in government acted separately without keeping an eye on what was actually necessary to get the job done. To ensure that everyone actually knows what collaboration looked like, they adopted a clear collaboration framework known as the “Three Ones” which meant that there is “one goal, one plan, and one monitoring and evaluation system” in place for better coordination across sectors.
Key interventions that make up the overarching plan include:
- Increase production and consumption of locally available, nutrient-dense crops.
- Increase small-scale livestock ownership.
- Expand irrigation potential to improve water-use efficiency and extend growing seasons.
- Improve water supply quality and quantity in households, health facilities, and schools.
- Improve access to hygienic sanitation facilities to address open defecation.
- Improve delivery of direct nutrition interventions through the public health system.
These priority interventions were also supported by each sector’s individual response to nutrition, some examples of which are outlined in Table 1.
Table 1. Key Examples of Sectoral Contributions to Nutrition
| Sector | Key Contribution to Nutrition |
|---|---|
| Ministry of Health | Strengthen and integrate nutrition-smart interventions (e.g., WaSH, environmental health, and health extension services) with other nutrition-specific interventions. |
| Ministry of Agriculture and Natural Resources | Pilot the establishment of 20 hectares modernized demonstration farms called Agricultural Innovation and Technology Centers. |
| Ministry of Livestock and Fisheries | Improve access to animal feed and support regulations that promote farmer productivity. |
| Ministry of Water, Irrigation, and Energy | Establish the Tekeze River Basin Authority to address the institutional vacuum for water resources planning and management. |
| Ministry of Education | Incorporate national school health and nutrition strategy in education programmes to better health and nutrition services for school-age children. |
| Ministry of Labor and Social Affairs; Ministry of Women, Youth, and Children | Improve the resilience of families in the Tezeke River Basin to economic shocks through the expansion of the Productive Safety Nets Program while improving the nutrition status of children as well as pregnant and lactating women. |
Building on Existing Collaborative Efforts
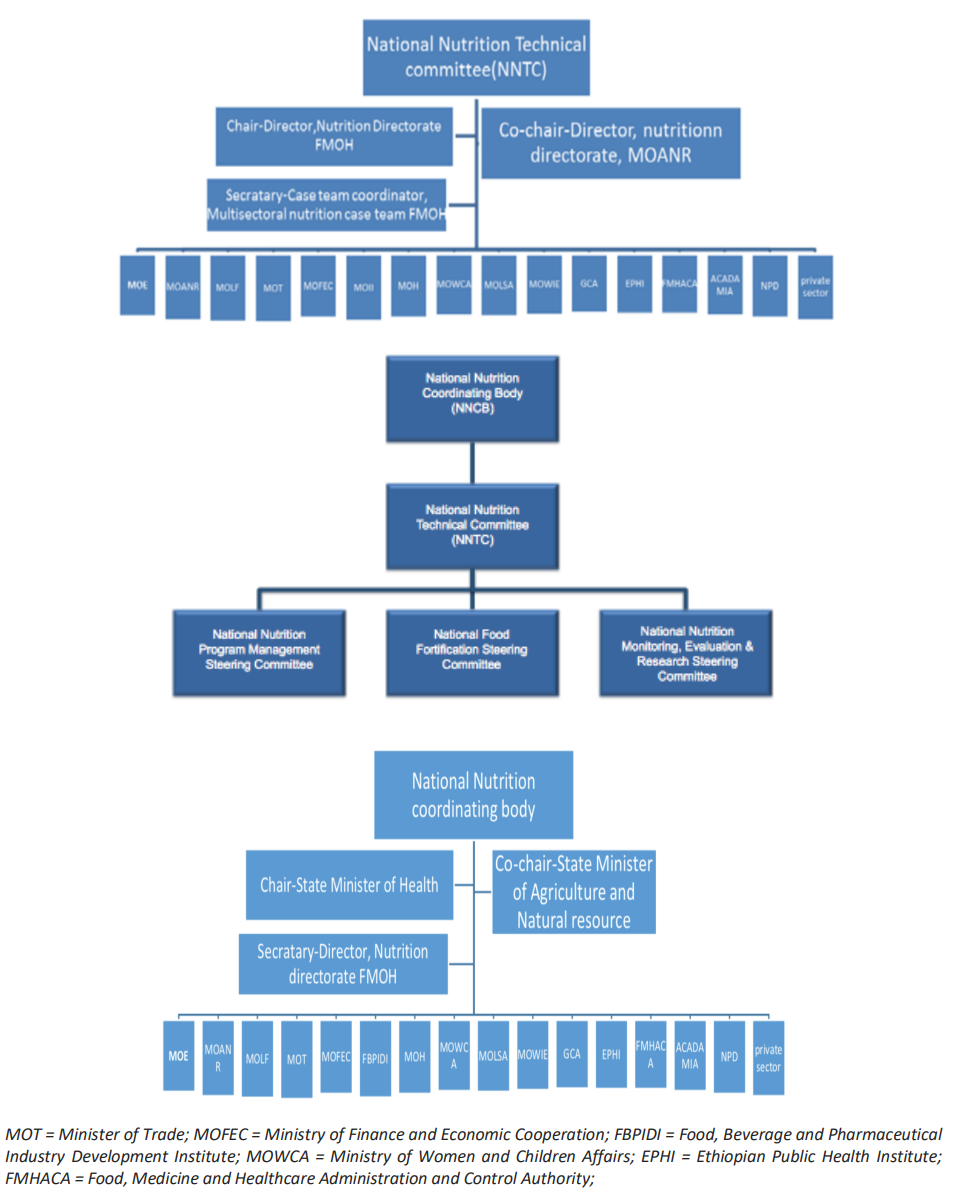
It was critical to build on existing government structures to catalyze progress. At the national level, multi-sectoral coordination is ensured by the two national nutrition committees, known as the National Nutrition Coordination Body (NNCB) and National Nutrition Technical Committee (NNTC). These two national entities have different goals as the NNCB is responsible for providing policy and strategic decisions related to the NNP. However, the NNTC works under the NNCB, and is responsible for the technical work related to the federal level NNP coordination.
At the regional level, there is a similar structure, known as the RNCB and RNTC. Figure 4 shows the level of integration and coordination built into the organizational structure below both the NNCB and NNTC.
Figure 4. Inter-ministerial Coordination Structure for both the NNCB and NNTC
Institutionalizing Flexibility and Coordinating Mechanisms
Traditional methods of governance and coordination, such as the top-down approach, were insufficient for this ambitious initiative. In fact, in the past, there had been concerns about issues related to the bureaucracy of government, which limited intersectoral coordination mechanisms to exist only horizontally at federal and regional levels. Moving forward with the Seqota Declaration, establishing entities with people from different sectors that would be fully dedicated to the initiative was required.
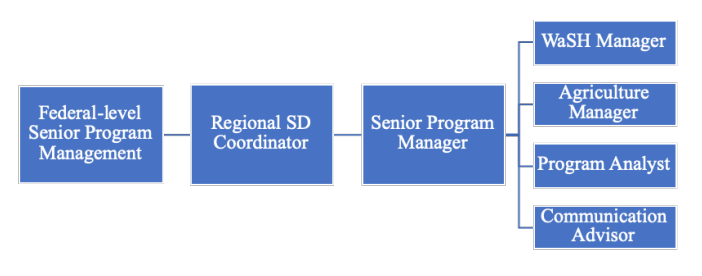
Thus, the creation of Program Delivery Units (PDUs), three in total, are a tangible “embodiment of intersectoral government.” PDUs are small teams of multisectoral experts placed in the federal, Amhara, and Tigray President’s offices to secure higher-level political commitment to regional nutrition activities, to ensure accountability to the highest level of the regional government, and to provide technical leadership and performance management support.
Figure 5 shows the composition of a single PDU and demonstrates how it can operate horizontally across sectors as well as vertically through different levels of government to ultimately form a team with diverse nutrition expertise proximal to executive power.
Figure 5. Program Delivery Unit (PDU) Composition
Innovating to Support Collaboration
Minister Admasu once said that “intersectoral collaboration is rooted in innovation” and that innovation relies on “learning by doing.” To this end, high-level delegations that traveled abroad to learn from other country experiences were able to bring back home some of the innovative ideas they learned and adapt them to the Ethiopian context. They realized that everything they learned could be translated to all of the sectors involved in the Seqota Declaration. For example, using technology to effectively manage water (i.e. Tekeze River Basin) would not only improve food productivity all year round (i.e. related to MOANR), but also increase coverage of safe and adequate water supply to households as well as the adoption of good hygiene through implementation of WASH strategies (i.e. related to MOH, & MOE). Improving water techniques was integrated through Agriculture Innovation and Technology Centers (AITCs), which provided the MOANR and its agencies with a platform to serve as demonstration sites for innovation. Lessons learned from the AITCs were intended to benefit MOANR directly but also with the expectation that new agricultural technologies would increase productivity and thus produce economic gains.
Monitoring and Evaluating Collaboratively
The “Three Ones” collaborating framework dictates that all nutrition-related monitoring and evaluation activities should be assessed under one integrated and unified system. The different sectors involved in the Seqota Declaration each have a list of key performance indicators that they are responsible for. These indicators are cross-cutting across sectors where relevant. For example, WaSH key indicators showed that the MOH needed to do more in terms of promoting hygiene and sanitation practices along with the MOE for targeted interventions at school. Another example is the dietary diversity score which falls under the health sector but baseline data showed that the score could not be moved by greater health promotion. This suggested that the score’s progress was being limited by factors controlled by other sectors such as the availability of diverse foods, gender inequity, or sociocultural factors.
With regards to monitoring, routine service and administrative records collected through sectoral information systems are used to provide information for timely monitoring, supervisory visits, and review meetings. Currently, the FMOH and UNICEF are working together on a pilot Unified Nutrition Information System (UNISE), a performance management tool that allows all sectors and partners to upload their targets and results so as to generate scorecards at the federal, regional, zonal, and woreda levels. This unified system is extremely important for progress towards the Seqota Declaration as it facilitates robust and continuous nutrition data management and becomes useful when seeking further investment. Dr. Sisay Sinamo, Senior Program Manager of the Seqota Declaration based in the FMOH, noted that having access to clear management performance indicator data during review meetings has allowed them (sector administrators and development partners) to make informed decisions at all levels.
With regards to evaluation, the Ethiopian Public Health Institute (EPHI) and Ethiopian Institute of Agricultural Research are charged with conducting official evaluations and undertaking “periodic assessments, operational research, and surveys to help identify program strengths, weaknesses, and key challenges.” Regional PDUs support this effort through the recruitment of data collectors and overseeing local data collection. Furthermore, regular “performance reviews” are part of the routine. The Deputy Prime Minister chairs quarterly meetings to assess the performance of all implementing sectors and development partners. The PDUs meet quarterly to share outcomes amongst each other and with relevant political leaders. Regional Presidents chair biannual meetings with regional actors and kebele and woreda administrators lead monthly meetings to share their performance with zonal and regional representatives.
Ongoing Collaborative Challenges
Today, approximately two years into the implementation of NNP II and the Seqota Declaration, it is clear that the NNCB has played an important role in bringing together various ministries. However, ongoing challenges with accountability and ownership persist – there is a persistent perception that nutrition is primarily a Ministry of Health (MOH) issue and that a lack of accountability across Ministries is the primary barrier to successful multisectoral coordination.
Even as nutrition has grown in national importance and public awareness, Ministry staff feel that with no cross-ministry reporting structures, there has been a lack of ownership and clarity about responsibilities for nutrition outcomes.
A separate but related challenge is how to improve coordination at the regional level. While many interviewees at the national level spoke about the leadership of the NNCB in nutrition governance, the Regional Nutrition Coordination Bodies (RNCBs) were rarely discussed. The function of the RNCBs in different regions appears to be variable, with ongoing work needed to strengthen them as coordination platforms.
A key component of accountability is the clear delineation of roles and responsibilities for all stakeholders. However, this role-definition for each sector is a challenge in the setting of multisectoral collaboration for nutrition governance. Deciding where the work of one Ministry starts and ends, and how it interfaces with other Ministries at the national, regional and local levels is a dynamic process with implications for political interests, leadership, budgeting, and accountability.
Key Takeaways
While Ethiopia is a unique context and has very specific cultural considerations, there are a few salient points which may be derived from this case and applied to a broader context:
- Making nutrition a national political priority is a key component of fostering multisectoral collaboration and improving nutritional outcomes. Though funds may be limited, political commitment and thoughtful programs can often attract donor organizations to contribute resources. Additionally, political pressure can help to drive budget decisions towards investment in nutrition.
- Multisectoral collaboration has contributed to a reduction in undernutrition rates in Ethiopia, largely due to the shift from nutrition-specific to nutrition-sensitive strategies. This approach is preferred as it addresses all determinants of nutritional status, including social and economic determinants.
- Accountability structures are vital to effective coordination, monitoring and evaluation in multisectoral nutrition governance. Multisectoral collaboration holds great capacity to improve population nutrition by simultaneously addressing multiple determinants of nutritional status. However, implementation and evaluation of coordinated efforts are difficult without accountability structures at the local, regional and national levels.
Overall, while challenges remain, collaboration from the initial development of the Seqota Declaration has allowed for more effective coordination across all sectors. Fighting a common “enemy” together is always more valuable and effective than doing it alone and without a clear agenda.
References
- World Bank Ethiopia Country Profile. Retrieved from http://www.worldbank.org/en/country/ethiopia/overview
- Ethiopia Profiles. Why Nutrition Matters? 2006.
- Ethiopia Demographic and Health Survey 2011. Central Statistical Agency, Addis Ababa & ICF International, Calverton, MD.
- World Food Programme. (2013). The Cost of Hunger in Africa: Implications for the Growth and Transformation of Ethiopia. Retrieved from
WFP Report - Copenhagen Consensus. (2014). Nutrition: What’s the smartest post-2015 target? Retrieved from
Copenhagen Consensus - European Union External Action. (2016). Implementation Plan (2016-2030): Summary Programme Approach Document. Retrieved from
EU External Action - Federal Democratic Republic of Ethiopia. (2018). The Seqota Declaration: Innovation Phase Investment Plan (2017-2020).
- Ruel M., Alderman H., The Maternal and Child Nutrition Study Group. “Nutrition-sensitive interventions and programmes: how can they help to accelerate progress in improving maternal and child nutrition?” Lancet. 2013;382(9891):536–551.
- USAID. (2018). Ethiopia: Nutrition Profile.
- WFP. (2013). The Cost of Hunger in Africa – United Nations World Food Programme – Fighting Hunger Worldwide. Retrieved April 29, 2019, from
WFP - Glandon, D., Meghani, A., Jessani, N., Qiu, M., & Bennett, S. (2018). Identifying health policy and systems research priorities on multisectoral collaboration for health in low-income and middle-income countries. BMJ Global Health, 3(Suppl 4), e000970.
BMJ Global Health - U.S. Department of State. (2018, August 10). U.S. Relations with Ethiopia. Retrieved April 26, 2019, from U.S. Department of State website:
U.S. Department of State - NNP. (2016). National Nutrition Program 2016 – 2020. Ministry of Health.